Young the Giant. Cough Syrup (right click to open in new tab)
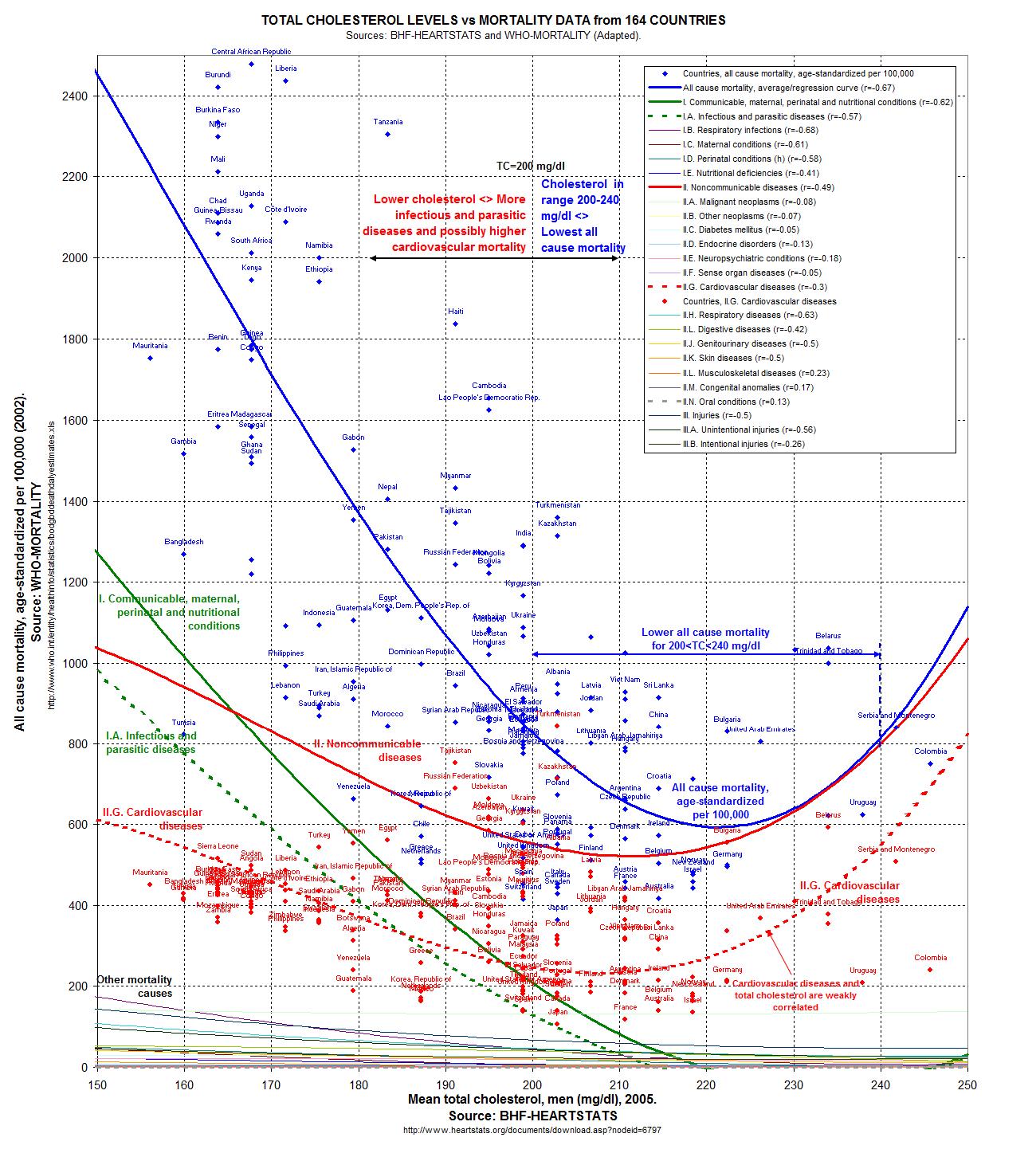
My thoughts are in response to a culmination of a number of recent news items in medicine. First, at the end of 2011, an expert panel convened by the National Heart, Lung, and Blood Institute recommended universal lipid screening in children 9-11 years of age and again at 17-21 years of age. On surface this seems innocuous enough… from a conventional medicine standpoint when one considers cholesterol to be an important marker of health. (Let's ignore for a little bit the fact that low cholesterol (along with exceptionally high) is associated with increased overall mortality in study after study after study.) No matter what, one of the most basic tenets of modern medicine is to consider the point of the test. If one runs a test, one must be prepared to do something with the information. If you aren't going to do anything about it, then why run the test in the first place?
I was pleasantly surprised by a JAMA editorial from earlier this month concerning these universal recommendations. The new NHLBI guidelines are linked to recommendations about both behavioral and drug therapies. The behavioral therapies are obvious -- increased exercise and a prudent diet (*cough*). And surely we should be recommending a diet focused on healthy, whole foods and avoiding processed foods for everyone. Healthy activity is also a universal and without too much controversy. But then you get to drug therapy for dyslipidemia, which in 2012 means statins for kids.
Here is where the JAMA editorial gets real. They note that in a meta-analysis of 10 primary prevention trials (primary prevention refers to people without prior cardiovascular disease, more or less the general population, whereas secondary prevention refers to drug treatment of folks who have already had a heart attack or stroke), statin use was associated with a 30% reduction in coronary events and a 12% reduction in total mortality (1). (Let's ignore the fact that these are relative risk rather than absolute risk numbers for now, more on that later!) Let's not ignore the fact that atherosclerosis begins in childhood, and that cholesterol levels track from childhood to adulthood. Reducing LDL cholesterol levels appears to extend the life of people with familial hypercholesterolemia.
But. But but but but but. Even a cardiologist would have to agree that most children with "dyslipidemia" will not develop early heart disease. Treating these children with statins exposes them to unwarranted risk and side effects. Drugs that lower cholesterol, such as fibrates, sterols, or the newer CETP inhibitors, are only associated with an increased or unchanged risk in cardiovascular events, suggesting that lowering cholesterol numbers itself is not a means to an end. The studies for the first CETP inhibitor, torcetrapib (which does a crackerjack job of lowering LDL and raising HDL at the same time! Whee!) showed a modest increased hazard ratio (only 1.25) which scarily enough would not have been detected if only the cholesterol measures were used, rather than overall mortality or cardiovascular events in the initial studies.
The JAMA authors go on to remark that statins have been tested in small numbers of children ( a few hundred, for studies ranging from 8 weeks to 2 years) for brief periods of time, and only the surrogate outcomes (cholesterol measures) have been assessed. So far, trials have lacked the size and duration to demonstrate any health benefits for children. If there are long term harms, it is unclear how these might be detected. Surely this uncertainly would be enough to give most pediatricians pause, to say the least.
So if one screens, there will be a compulsion to act quickly on the results. Do you give statins to children with NO data? Wouldn't you recommend whole foods, avoiding processed garbage and prudent exercise as staples for all children as a matter of course? "What this novel public health intervention in children clearly lacks is an evaluation to determine whether the long-term risk-benefit profile may in fact be favorable or harmful."
Let's move on from children to women, where statin use has also been controversial, as a very new meta-analysis was published in the Journal of the American College of Cardiology this very week: Meta-Analysis of Statin Effects in Women Versus Men. I imagine this study will be used in order to further pressure all of us with average cholesterol to go on medicine for primary prevention of heart disease. This meta-analysis (which brings together the data from a number of different studies) strives to do what no statin study has done before--prove any benefit in women, particularly in primary prevention. In the end the authors find in a compilation of data from 18 trials with sex-specific outcomes (141,235 people and 40,275 women) that outcomes were similar for women as for men. That is a statistically significant benefit for women as well as men of similar magnitude in both primary and secondary prevention. All-cause mortality was also lower with statin therapy both in women and in men with no significant differences between the sexes.
Well. Hallelujah. At last. The conclusion: "Statin therapy should be used in appropriate patients without regard to sex."
Of course, as we all know, the devil is in the details. And in a beautiful editorial in the very same edition of Journal of the American College of Cardiology we have "Controversy and Consensus About Statin Use: It Is Not About the Sex." The editorial says, yes, indeed, finally, and it is no surprise, that statin therapy should be of similar benefit to women and men, but what does that mean, exactly?
It means, with secondary prevention, those who have already had a heart attack for example, that statins do indeed impart benefit, and I'm willing to extend that benefit to women as well as men. But when we come to primary prevention (statins in people with risk factors for heart disease, not proven heart disease), we are talking a whole different kettle of fish.
First off, of more than 2300 studies identified by the doctors doing the meta-analysis, only 18 met all the inclusion criteria (meaning they were of high quality enough to be included). 8 were primary prevention trials, and 17 were funded by the pharmaceutical industry, and only 2 included sex-specific data on side effects (or "adverse events"). One of the included trials was JUPITER, which remains controversial as it was halted early and had a short follow-up.
The "devil" here is that women are considerably less likely to die of heart disease than are men. Thus any primary prevention in women will need to meet a more stringent requirement than in men, as by numbers alone primary prevention of heart disease will be of lesser benefit in women. The risks of diabetes, muscle problems, cognitive deficits, and perhaps increase in cancer would be expected to be more of an issue in women, with smaller lean mass thus higher relative statin dose (same issue is at play in children), longer lifespans and lower risk of heart disease and higher risk of cancer than men. While "relative risk" of decrease in heart disease (say a decrease of 2% to 1%, with a relative risk decrease of 100%!) might be promising, the absolute risk (that change from 2 to 1%) is unimportant. So here we get to the heart of the matter:
Women without CVD have lower annual mortality risk and lower CVD risk than men without CVD. Therefore, the absolute benefit of statins will typically be less for women than men, suggesting it might be appropriate that women receive statins less frequently than men in the setting of primary prevention. The current meta-analysis provides information about sex-specific relative risk benefit and not absolute benefit. Both absolute risk of CVD and the proportionate risk reduction associated with statin therapy are needed to make informed clinical choices with regard to the use of statins for primary prevention. Although the latter might be similar for the sexes, the former might be quite different.As only 2 studies provided sex-specific risk data, we simply cannot evaluate the risk of statins for primary prevention in women Adverse outcomes are extremely clinically important when we are giving medicines to healthy people to prevent disease. More wisdom from the editorial:
Sex-specific results in cardiovascular prevention tirals should be provided for relative and absolute benefits, adverse outcomes, and cost-effectiveness. Only then we will know with less uncertainty whether what is good for the gander is also good for the goose. Medicine is still an art. [emphasis mine]And, finally, some thoughts on some email conversations I've had with Kurt Harris on low dose naltrexone. We were discussing the use of LDN in allergy and autoimmune disease, and I had stumbled upon this skeptical webpost: Low Dose Naltrexone, Bogus or Cutting Edge Science? The truth is that LDN has shown a robust benefit for a very challenging illness, Crohns Disease, in studies at Penn State (2). In these studies, the inexpensive and by any rational observation low risk low-dose naltrexone performed better than the incredibly expensive noxious anti-TNF-alpha Humira. We certainly know much more about Humira's risks-- they are many, and yet it is somehow dangerous and "woo" to recommend a trial of LDN in comparison. LDN has real potential to modify the immune system to decrease deadly and intolerable immune reactions in diseases such as Crohns. Naltrexone has been in use for a decade or more, and while there is a dose-dependent risk of liver damage, that risk tends to happen at 150mg daily. LDN is about 4.5 mg a day. Sure, there is no argument that we should have more data, but how is it crazy and dangerous to recommend LDN for Chrons (as opposed to Humira or even steroids) and not crazy and dangerous to recommend statins for primary prevention, a very accepted practice?
In my mind, when we are considering difficult illnesses with only dangerous evidenced-based cures, we have consider common sense and the cost of large trials and the corrupt influence of money and the pharmaceutical industry. One such example is the vitamin supplement SAMe, which performed better in trials at MGH than any FDA approved adjunctive treatment for resistant depression. SAMe is not without risks (mania and elevated homocysteine), yet surely Abilify (which has FDA approval), 10X more expensive and with risks of permanent movement disorders, weight gain, metabolic syndrome, and diabetes should sensibly be a second-tier option in resistant depression compared to SAMe, with a decades-long track record of randomized controlled trials? Somehow that is not the case. Somehow we put Abilify ahead of the mere supplement.
I'm preaching to the choir. But I suppose that is what a blog is for. The papers march on, the money, the meta-analyses, the editorials. Does anyone demonstrate common sense in actual clinical practice? We shall have to see. Money (and time?) is running out for us to come to our senses.
(I read recently The Cholesterol Delusion by Ernest Curtis, M.D., a cardiologist, at the recommendation of Mike Eades. It's a short read, pointed, and interesting. Worth the time. One of his most important points of wisdom is that any study or news report touting relative risk in lieu of absolute risk has an agenda and is trying to make a dramatic statement when there may or may not be any reasonable difference in risk.)



{kind=link}