Anyway, the research team at Massachusetts General Hospital (I attended some of their meetings when I was a resident) just published a good paper in the Journal of Affective Disorders: Second-tier natural antidepressants: Review and critique. This paper goes over R. rosea, chromium, 5-HTP, and inositol, but I'm going to start with inositol, as I could use some second messaging review myself, and I looked it up specifically for a patient as well. Even though we are talking "natural" supplements here I still don't contend this is "evolutionary" psychiatry - none of our ancestors were chugging vats of inositol so far as I know - but figuring out how these things work helps us to understand biochemistry and speculate as to what could be going on that we might end up with an inositol deficiency, as it were.
First off - let's just mention the "first tier" natural antidepressants and complementary medicine treatments. That is, stuff generally considered "herbals" or "alternative medicine" that has a solid evidence base in the scientific literature. (I'm using the "quotes" because I don't see the need to distinguish these things so much - is there evidence base or not? I don't care if someone thinks meditation is flakey or "new age" - does it work? It certainly can! With life-changing results. Off my high horse). The well-studied "herbals" with a "growing consensus of antidepressant effectiveness and safety" include St. John's Wort*, SAMe, and omega-3 fatty acids. Folate, acupuncture, and exercise are other alternative treatments that have some studies of efficacy as antidepressants.
So, inositol doesn't have as much evidence base as any of the treatments in the previous paragraph, but we'll talk about what it is, and the evidence we have. (SAMe has shown efficacy in at least 20 trials over the years, some larger than others, some better controlled than others, so it is my "favorite" alternative treatment - but it can cause mania, and unless your folate cycle is humming along, can become evil homocysteine, so be warned).
So - inositol is a sugar alcohol and an isomer of glucose, and its 9 varieties are found mostly within cell membranes. Myo-inositol is the most abundant stereoisomer, making up 95% of the total free inositol in the body. Humans generally consume about a gram of inositol a day, and it is abundant in grains, beans, nuts, and fruits. (You might not be surprised to know the best sources are organ meats - beef heart and liver, but also wheat germ - but, uh oh - wouldn't the phytic acid in wheat germ bind up inositol - well, inositol is a part of phytic acid, which we can't actually break down, so, typically, animal sources will be more bioavailable than the phytate plant sources of inositol.) However, I ain't gonna lie - we can make inositol from glucose, and there's no evidence that we have a limited capacity to make inositol so that a dietary deficiency may not matter. We eat maybe a gram a day, and our kidneys make about 2 grams a day. Inositol is sometimes called "Vitamin B8."
So what does inositol do in the human body? Well, tons of things, actually. It is a key part of the second messenger system. Que? Well, in the pony express line that is a cell, surface proteins and receptor complexes (the mailer) hand off signals to the second messengers (the riders on the ponies) who pass the signal along eventually to other cell systems (the message recipients), such as the nucleus. All the major neurotransmitter systems use inositol as part of their messaging line - I'm talking dopamine, norepinephrine, serotonin, acetylcholine… "The potential importance of inositol in psychiatric disorders is thereby evident when one considers the number of receptor types/subtypes that interact with this signal transduction pathway."
Biochem nerds will already know this next bit, but biochem nerd wanna-be's listen up (the rest of you can skip to after the picture, because this bit is a little dry) => Inositol is used to make inositol triphosphate (IP3) and diacylglycerol (DAG). IP3 binds IP3 receptors, particularly calcium channels in the endoplasmic reticulum, which will cause calcium levels in the cytoplasm to increase, causing a cascade of intracellular activity. Calcium and DAG can activate protein kinase C, which (as all kinases do) goes around sticking phosphates on things, leading to altered activity. Anyone learning molecular biology and biochemistry will see this pathway mentioned so many times your eyeballs will glaze over. So, in short, inositol is vital.
Picture! (from wikipedia):
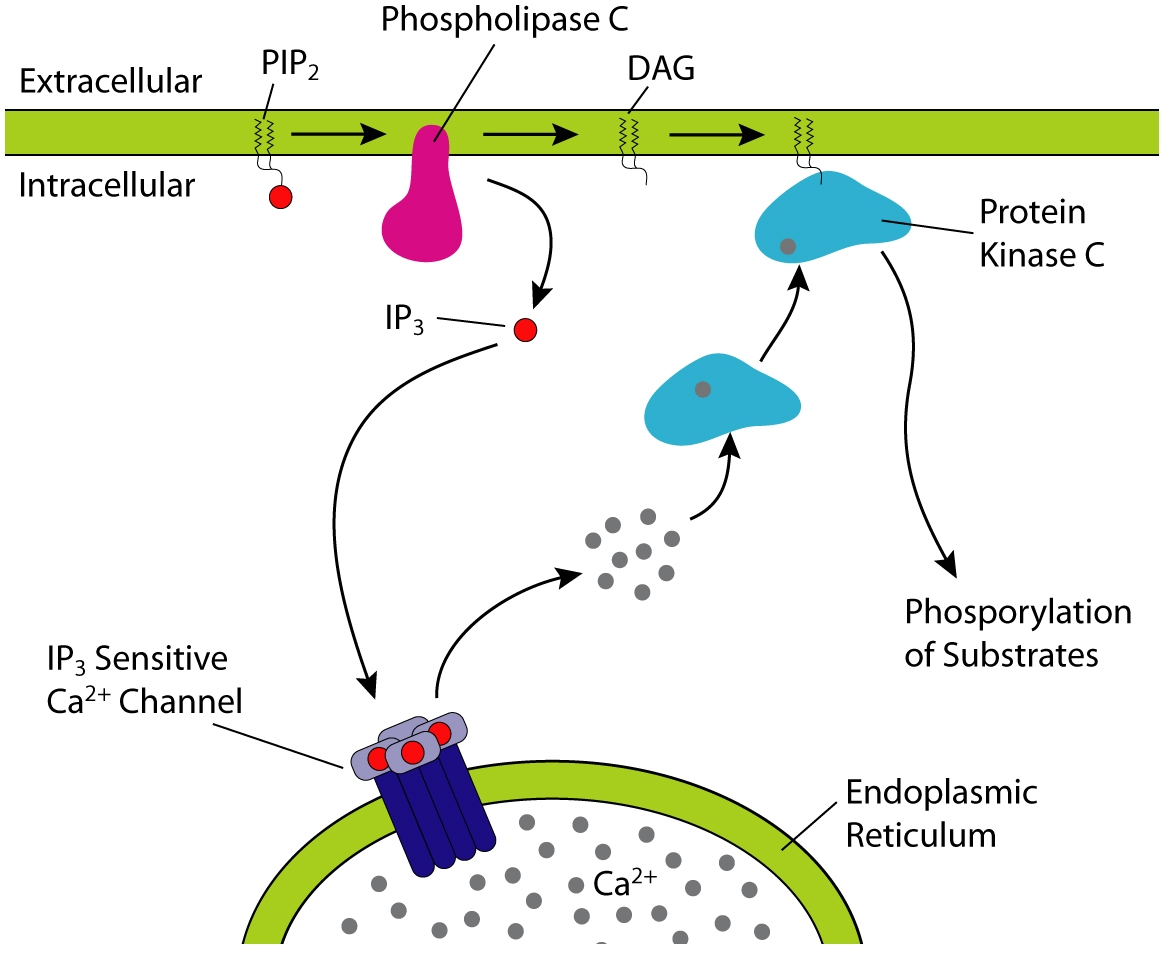{kind=link}

There has been discussion in the comments on my lithium posts about lithium interfering with inositol metabolism - specifically it interferes with inositol monophosphatase possibly leading to reduced recycling of inositol and IP3 in the cell and reduced inositol levels (1) however - it is unclear that the actual end product is a reduction of second messenging or something else. One theory of bipolar disorder is that it is caused by "hyperkinetic second messenger systems." This imaging study seems to confirm that something screwy is going on with second messenger systems in bipolar disorder, but no one is sure yet what the heck it all means. By this same theory, the "depression" side of bipolar disorder might result from a reduction of inositol after the manic episodes, and depressive disorders might result from reduced signaling in the first place, leading to inefficient cell energetics, mechanics, and build-up of toxic calcium in the wrong places at the wrong times. Sounds nasty.
Ready for the clinical data (ie the really interesting and more practical stuff)?? A study back in 1978 found decreased inositol levels in the spinal fluid of depressed patients. However, subsequent studies didn't replicate the finding, and that levels of inositol in the spinal fluid didn't predict response to inositol. But post-mortem examination of suicide victims have shown lowered myo-inositol levels, and magnetic resonance spectroscopy showed reduced myo-inositol levels in the frontal lobes of bipolar and unipolar depressed patients. Dietary administration has been shown to increase inositol concentration within the central nervous system in humans (2).
But does it work? In the comments, more than once people have mentioned taking inositol 750mg several times a day with good effect. Well, there are a number of trials, some controlled, some open-label. In the trials, an average dose was 12 GRAMS a day (which would be 16 of those 750mg capsules - divided 2-4 times a day - which would mean you would go through this bottle in a little over six days, putting the monthly cost minus shipping at about $34… inositol is also available as a powder which seems like it could be a bit more cost-effective for the "prescription" doses studied). Some trials showed no benefit, but others showed no improvement at 2 weeks, but a definite improvement at 4 weeks. Trials (as an adjunctive treatment, meaning with mood stabilizers) in bipolar depression were a little more promising. One patient did develop mania after 24 weeks on inositol. Most of these studies were done on people who did not respond to traditional antidepressants, and so even a modest effect is promising, as so-called "treatment resistant" patients tend to be "treatment resistant" to all kinds of interventions. Additional studies (typically using even more inositol - 18 grams a day) had positive results for anxiety, bulimia, and obsessive compulsive disorder. Inositol seems to act on these disorders a bit like nature's SSRI.
What is inositol's downside (besides needing to take mountains of it) - side effects in these trials included mild increases in plasma glucose, gas, nausea, sleepiness, insomnia, dizziness, and headache, and then there are the case reports of mania (any antidepressant, including light therapy, can cause mania in vulnerable people.) No one dropped out of the trials due to side effects from inositol. Inositol does not appear to have any drug-drug interactions - however, it might induce uterine contractions in pregnant women, so should not be used in pregnancy (3).
In the end, inositol might be helpful for some people, and it would be interesting to see if the organ-meat eating paleos have higher inositol levels in the CNS than your average grain eater. But you'd have to eat a lot of beef heart to reach 12 grams daily.
*about St. John's Wort - product studies I have seen in the past suggest you are unlikely to get standard doses or product in SJW off the shelf, also it is most probably an MAOI and definitely has major drug interactions, such as with birth control pills and coumadin - SJW is not a product I routinely recommend for those reasons - BUT in the RCTs of pharmaceutical grade - one of which was done by this same Massachusetts General Hospital research group- it worked as well as prescription antidepressants. Chris Kresser suggests that this is because they all work as well as placebo. Personally I think from reviews of published and unpublished studies prescription antidepressants give you a 10% advantage over placebo in the short term and likely work better in the long term, but they are a pain in many ways, have side effects, and the long-term effects are generally unknown… my favorite source for unbiased evidenced-based information on psychiatric meds is Dr. Daniel Carlat his team at The Carlat Report. He has a great blog focused on industry influence and sniffing out misleading information but it is geared more toward psychiatrists than the layperson.
Nice! It's great to see some serious research on micronutrients and mood disorders emerging. Even before I started thinking about the science of it I already thought that there might be something about diet that could alter moods since drugs alter moods and they're all just chemicals in the end. A deficiency in what is required for normal functioning sounds more plausible than a drug or Buddhism deficiency to me. We haven't evolved to be mopey and sit in our rooms listening to Grunge albums and reading Nietzsche - we evolved to LIVE and be enthusiastic about it, and to need to consume various molecules to function properly.
ReplyDeleteI'm pretty convinced of the efficacy of the previous nutrients you've covered. Looking forward to the upcoming posts. Cheers.
glad to hear SAM-e is (or has become) one of your fav alternative treatments for depression :)
ReplyDeletealthough i reacted brilliantly to it for the first few months, it stopped working completely afterwards, which is a bit sad, because as i mentioned earlier, it provided the highest quality mood enhancing effect of all supplements i've ever tried. must be the folate cycle or something as you mentioned (i seem to have a slightly elevated homocysteine level of 11, which may be related). however, i tried taking methylfolate and B12 to see if it could re-start the SAMe, but to no avail. no effect anymore what so ever. any idea why? (i send you some swiss dark chocolate if you can resolve this chemical riddle ;)
wrt inositol: even just 500mg has a pronounced effect on me. it has relaxing, anti-anxiety and mood enhancing effects for a few hours. like so often, the leakiness of the BBB might play a role, as the transport and diffusion of myo-inositol seems to be limited (http://is.gd/LP9hma).
in other news, i'm currently a big fan of krill-oil. mercola seems to be right, when he says it's way superior to fish oil. in my ecperience its about 4-10x as effective per DHA/EPA content. also has stronger focus and mood enhancing effects in general (plus a ton of brain, skin, and eye-protecting astaxanthin as a bonus. it's basically impossible now for me to get a sunburn).
btw, did you already do a post on P-5-P? also one of my fav (and strong) brain and mood-enhancing supplements (50-100mg before breakfast). this stuff never fails. has a similar effect as modafinil or ginseng with regards to brain-boost effect and enhanced focus.
forgot to mention another benefit of krill-oil i noticed, and didn't quite believe before: the anti-inflammatory effect is crazy. as in, surprisingly strong. two small softgel pills manage to suppress my chronic neck pain by about 90%, which is about the equivalent of one aspirin tablet. think about this for a second! we all know how effective aspirin is in preventing heart attacks. so what if krill oil has the same, potent anti-inflammatory and blood thinning effect (which it has) as aspirin, *without* the negative side effects? whoa. and maintenance dose for me is only ONE softgel a day. that's an excellent deal if you ask me..
ReplyDeleteI just want to let you know how much I enjoy your analysis and explanations. I think the information you present here is fascinating on a number of levels. I especially enjoy learning about chemistry while reading about a supplement. :-) Thank you for the work you put into this.
ReplyDeleteBig thank you from me too, as I also enjoy reading your blog.
ReplyDeleteYour discussion of inositol reminded me of a popular supplement to combat Polycystic Ovarian Syndrome, d-chiro-inositol. It seems to ameliorate some metabolic abnormalities associated with PCOS (I haven't tried it). I wonder if inositol has an anti-dpressive effect through mediating the "metabolic abnormalities," like sensitizing one to insulin.
Here's the paper on treatment of PCOS with it: http://www.ncbi.nlm.nih.gov/pubmed/15251831
Thanks again! : )
Hey loved the post!
ReplyDeleteJust wanted to point out that although inositol is an isomer of glucose (they both are C6H12O6) its pretty whacky because it doesn't have an oxygen in its ring! I remember a few years ago coming across it in my biochem textbook and thinking it was a typo.
Anyways, seeing the title brought back my memory if that moment.
Best,
Nick
Inositol has greatly helped my depression, it really works. It has completely and totally reduced my mood problems.
ReplyDeleteI've never had any sort of manic reaction from inositol, and I do tend to get some degree of manic reactions from anything that can trigger mania (sleep deprivation - yep, mania... bright light - mania... season change = mania, most anything that elevates mood = mania).
IN spite of the fact I typically get some type of manic reaction from antidepressants, inositol has never done this for me. What it HAS done is even out my day to day mood variability. Prior to using inositol I would have oscillations in mood over 2 or 3 days, where I might be kinda high (or not that depressed), and then I would have 2 or 3 days where I would be kinda low (or very depressed). The 2-3 day mood oscillations typically interacted with my baseline mood state, whether I be doing well, depressed, or what not.
After taking inositol (about 5 grams per day in 2 divided doses) that day to day mood variability has smoothed over and my mood is much more consistent day to day.
It feels as if I had a car which badly needed a wheel alignment, and inositol has given me smooth steady control over the car ;D
However, as for my WEEK TO WEEK or MONTH TO MONTH mood variability, inositol has not done anything to help that. I still have weeks and months where I am "high" and weeks or months where I am "low".
All in all I feel more functional and sane now that I am not laughing hysterically tripping on my mind one day drawing frenetically and feeling like I understand everything, but then 2 days later I am crying in my car feeling like it is hard to move my body and thinking. Yea, that's a good thing I don't have that problem anymore, I was way lower functioning then.
I have no idea why inositol has smoothed out my moods day to day, but it's frigging awesome.
I also used to get this problem where, at night, my mood would nose dive and I would get crazed and agitated and chaotic, like my head would be full of noise and pain and I would just be freaking out. I would have intense negative thoughts and my mind would just be noisy and painful no other way to describe it, it felt like HELL. Since taking inositol, this almost never ever happens anymore, ever. I used to get these hell trips like, a few times a month, now I get them a few times a year.
The ironic thing is that, prior to discovering inositol I had consulted with a psychiatrist. They gave me abilify for my "bipolar II disorder". The abilify was horrible. In addition to eliminating natural happiness and natural negativity, it EXACERBATED the up and down of my mood (as opposed to being up and down 2-3 days I was up and down every other day). The "hell moods" also became much, much more common and worse and unbearable. I quit abilify cold turkey, which on the 3rd day of withdrawal had me pretty damn high for 2 days, which quickly turned into a month of depression.
Shortly after dumping psychiatry I found inositol, and I can't help but think it is so ironic that this OTC vitamin has done so much to help my mood whereas the psychiatrist was completely and totally useless.
I never thought the "hell mood" thing would go away, I never expected it to, I am amazed that this vitamin has freed me from it.
I still get them, but its super rare.
I found it very interesting reading your post about moods and up and down. I've never been to a psychiatrist, and nobody except one psychologist thought I might have bi polar. I sort of wonder as well in my case, whether some times of the month I feel more of a high, and then anxious right before the time of the month, and two weeks later I might feel high again. It's not always that precise.
DeleteI've been using sam e since beginnning of last year. Just when I thought it had stopped working and had started to decrease how much I take it, I needed it again. I took it on an empty stomach which I had stopped working, and within an hour helped my horrible dark mood on christmas morning. The horrible mood was making my anxiety worse.
I've bought Inositol in powder form and now I'm thinking of trying it when I feel low, as opposed to now when I'm on a high.
I literally got a chill when I read "...I am crying in my car feeling like it is hard to move my body..." and "...at night, my mood would nose dive and I would get crazed and agitated and chaotic...". Could've been me saying that and I've always been befuddled about the nighttime thing. I tend to label myself as "melancholy"; doctors along the way have suggested that I'm depressed but I never bought into that. Since I've been reading so much lately I much more identify with the idea of an uneven mood than a pure diagnosis of anxiety or depression. In once again seeking help for whatever is "off" with me I went on ADHD meds (Vyvanse) last September. The euphoria they induce is a definitely plus and the increased focus has made life less overwhelming. However, I have noticed a definitive cyclical mood change which has now been diagnosed as PMDD. I honestly think that it's been PMDD causing most of my issues all along and, the ADHD may be present, but most likely not necessary to medicate. I also follow a low/no carb diet and drink a crap ton of caffeine. So between the increased dopamine, lack of carbs, and high intake of caffeine I'm pretty sure that I've depleted whatever serotonin that I had (which was probably low my entire life anyway), and have also negatively impacted my GABA. So the next step, according to my doctor, was to add Prozac into the mix. Ummmm, yeah... No. So that prompted a whole ton of research on my end that led me to amino stacking, along with inositol, P5P, and magnesium. Literally the day after my birthday I sat in my car for almost 3 hours in a parking lot crying and kind of unable to move. Of course that would've been at the height of my PMDD cycle. The next day I started the supplements and I definitely feel clearer but I can also feel a bit of the PMDD symptoms starting to creep in. The end of next week will begin my 6 days of hell, so by then I should be able to gauge how well my dosages are working. I'm only taking 750mg of the inositol at bedtime and I suspect that I will need to increase it even if only during the worst part of the cycle. That's how I cam across this post and your comment. I'm so happy to hear such great things about natural resources that are available, and I hope that people continue to study, document, and share the benefits so that the rest of the population realizes that there are more cost effective, non-synthetic alternatives that they can explore.
DeleteInteresting.
ReplyDeleteResearch suggests inositol causes mania and may be fundamental in bipolar. I've been dxed with that and yea, it might be true, it might not be... like I said I get mild manic reactions from FLAX OIL from LIGHT THERAPY from SLEEP DEPRIVATION from SEASON CHANGE , and from most mind altering substances... but I have never had a problem with inositol. Weird. If anything it has helped even out my mood at least on a day to day basis.
I would expect a bipolar person to have much more of a problem with light therapy or with sleep deprivation, than with inositol. Most bipolar people naturally go manic in the spring or summer, right? Light + sleep deprivation is basically triggering an artificial season change.
Speaking personally, any relative increase in light will make me go nuts at least temporarily. Absolute level of light is not as important as 1) trend of light (e.g. later, earlier) and 2) relative amount of light (e.g. more less). I think back to march, when the light increased just a bit. I had one of those really bad "hell moods" at night, and then I woke up the next morning quite early after 4 hrs of sleep feeling high as a kite like I had taken the best drugs. Then I spent the next few days feeling elated and excited over nothing, drawing fitfully, being creative, being more confident and less anxious and more silly and humorous, and feeling just so awwwesome... and then it sorta went away after a few weeks. Poof thats it, totally gone.
At the time I was also increasing flax oil (which I know promotes being high), so I had 3 triggers working together.
Clearly triggered by a relative increase in light from spring, plus sleep deprivation.
But inositol has never done anything "bad" or "weird" to my mood and it has only done good things. Hmmm.
What I experience does seem to be somewhat related to bipolar disorder, but inositol is the one manic trigger that never does anything and only seems to help. *shrug*.
qualia - as another cray cray person, it has been my discovery that nothing mood boosting lasts for long, it always poops out to some degree.
ReplyDeleteYou have to consider that no one is depressed because of a lack of sam-e, or a lack of zoloft, or a lack of black tar heroin. There are other reasons people are depressed but most depression cures are just a bandaid fix which add NEW abnormalities, to an already abnormal situation.
The brain has an incredible ability to keep balance and adapt to abnormal levels of neurotransmitters or what have you, and if you flood your brain with a bunch of stimulants, your brain down regulates those target receptors and viola the drug poops out after a few weeks. We are not meant to take wellbutrin and abnormally increase the level of dopamine in our brains. Our brain will respond via downregulating the target receptors and other changes.
Rarely does a drug poop out completely, usually it only poops out partially. If I increase my caffeine consumption by 2 cups per day, I will be flying high with energy, running around feeling super wired and stuff, but after a couple days of that, the caffeine will have a minimal effect. Why? My brain has adenosine receptors, and they decrease in response to the caffeine. As a result, plowing myself with caffeine no longer works to make me feel really smart and energetic and clear thinking and motivated the way it used to. Then I just feel blah, and I would have been better off NOT increasing my caffeine intake that much because it all evens out to the same level of responsiveness whether you are drinking 1 cup or 10 cups daily.
A few years ago a small coffee per day had a big effect on me.
Today I can drink a 32 ouncer and barely feel it, all it does is take away the withdrawl and give me a short lived mild boost. I could always drink more coffee but, we all know whats going to happen, I'll just have an even worse caffeine addiction once the tolerance sets in.
Antidepressants of any kind are just like that.
The only antidepressants which don't poop out are those which are curative, stuff like leptin (which rebuilds the brain) and stuff that helps organize the stress response (which destroys the brain) or depressions which are reactive to specific deficiencies (e.g. a deficiency of thyroid hormone will cause some types of atypical depression and taking thyroid hormone is curative in this case). Severe omega 3 deficiency may be curative considering omega 3 deficiency is a direct cause of depression, I have hope that flax oil won't poop out on me and will prove "curative" as opposed to a temporary fix like most antidepressant interventions.
Katya -
ReplyDeleteInositol also sensitizes serotonin receptors.
The main reason PCOS is helped by d-chiro-inositol is because PCOS women have a specific abnoramlity where they do not synthesize enough d-chiro-inositol. D-chiro-inositol is a metabolite of myo-insoitol (there are many inositols, you know) and PCOS women don't do this well, probably genetic variability.
D-chiro-inositol is fundamental in the ovulation process - that is to say the actual process of follicle maturation and rupture requires this molecule. The fundamental defect in PCOS is an inability to ovulate in spite of ample hormonal stimulation (high levels of LH and FSH). For some reason, women with PCOS don't ovulate, instead the follicle becomes cystic and the cycle is arrested in the mid follicular phase. Multiple cystic follicles develop and the secondary hormone imbalances are thereby exacerbated (high levels of testosterone and estrogen) . A new cycle develops, a pathological one, of high gonadotropins, unruptured cystic follicles (inability to ovulate) and high sex steroids as a result.
D-chiro-inositol does not help PCOS because it is insulin sensitizing, it helps because it allows them to ovulate normally. Glucose disorders do not cause PCOS, they only worsen or trigger it. There is an underlying vulnerability to abnormal ovulation. This is why many women are fantastically obese and diabetic but never get PCOS - you need the specific genetic predisposition for it.
I also have PCOS so perhaps the reason inositol helps me so much is because I may have a genetic inability to synthesize enough of it, which then predisposes to PCOS.
This inositol which has been used in studies, is that plant based or animal based?
ReplyDeleteYou said, "so, typically, animal sources will be more bioavailable than the phytate plant sources of inositol."
Just wondering if the Paleo heads will really need to eat lots of beef hearts. Do they really need to achieve 12 grams of inositol for the benefits you outline?
And do natural sources of inositol induce mania (in vulnerable people)?
ItsTheWooo2,
ReplyDeleteThanks for your in depth response. I suppose I could have read the paper more thoroughly before commenting! What you wrote is in agreement with my experience: even after turning to a traditional/paleo diet, my LH/FSH ratio is still off (though improved), indicating to me that better blood-sugar regulation is not sufficient as treatment.
However, I have to disagree that so many of us (1 in 10-20) “have a genetic inability to synthesize enough of it.” As is true for all diseases of civilization, I doubt that such a large fraction of the female population is (even slightly) genetically unfit. Perhaps I am conservative, but I believe that DCI supplementation is only a temporary solution to a problem with an existing solution (perhaps it is specific nutrient related, or sleep cycle related; my bet is that it is linked to gut flora, as certain ones can produce DCI.) More recently I’ve been worried that I caused more permanent damage in my teens with poor sleep/diet, but I am optimistic about trying the GAPS diet.
Regardless, I am glad that DCI is working for you; perhaps I will try it, too. How lucky are we to live in an age when pubmed and blogs like this are at our fingertips??
I don't know how they make inositol in the studies - it's basically a type of glucose. In plants it comes attached to other stuff as part of phytic acid, which we can't break down, or sometimes it comes as part of lecithin, which we can break down. I'm guessing the supplement is plain old inositol, not attached to anything,
ReplyDeleteI'm guessing no people in the history of the world ate enough beef heart to get the kinds of doses of inositol we are talking about in these studies. We make plenty of inositol as well - twice as much as we eat, and we can make it easily in the kidneys from glucose. I don't know why some people are low, and it *seems* to be linked to depression - like the PCOS issue Woo was talking about - maybe some people are genetically bad at making inositol, and they might benefit particularly from a supplement.
Since natural sources are such a low "dose" I don't think we need to worry about mania too much from beef heart or liver.
I think the high doses were used in the studies because it took a considerable amount to induce inositol changes in the CNS (70% increase with dose of 12 g daily in humans in the Levine paper from 1993 I believe). Qualia and Woo use much lower doses and seem to feel a benefit from it - Qualia suspects she has a leaky blood brain barrier, but none of the studies had doses anywhere near that low - the lowest was 5g (if I'm remembering correctly) and no effect was found from that amount. So I haven't reviewed literature of inositol in lower doses.
I'm not recommending inositol so much as using it as an example and learning a bit of biochem from it. No one knows the long term effects of taking 12 or 18 grams a day of the stuff, after all.
(I should say I am not recommending inositol as a supplement for general use - most of us probably have plenty of inositol even if we have crappy diets, because the person with the crappy diet is sure to eat glucose! - given the relatively cheap cost, the seemingly benign side effect profile, and novel mechanism of presumed action, I can see how it would have a place in a psychiatrist's armamentariam - especially for someone who prefers natural treatments or hasn't responded well to other treatments and lifestyle changes. Supplements, not being pharmaceutical grade (usually) can be tricky.
ReplyDelete(but outside magnesium and vitamin D (if you are low) I'm not a big supplement recommender anyway - if you eat grass fed beef liver and seafood you should be covered for the most part. If you don't, a good multi mineral is a safe bet. (i actually get a pharmaceutical grade one from Designs For Health for weeks I dont eat liver ) If you are low carb, you might want to add some vitamin C and run the diet through fit day or something to check out the potassium and other nutrients.
ReplyDeleteBut - one of the most interesting things about the Dietnand Violence papers is that the dietician-designed diets gave the prisoners their RDA for almost all vitamins and minerals (and Gesch even took care to measure what prisoners actually ate, not just what they were served) - but they still benefited from the multivit,mineral, and EFA supplement, which presumably topped off their micronutrients.
ReplyDeleteBut of course a paleo 2.0 diet will no doubt be more micronutrient rich than a prison food pyramid diet.
Anyway, something to think about.
(1) "There are two circumstances in which I tend to see heavy pot use"
ReplyDeleteBut you wouldn't be seeing the successful and happy ones.
(2) "does cannabis use increase the risk of schizophrenia use or what?"
The problem with all these studies is they are studying a population of cannabis users eating a Neolithic diet. There could be no effects, or even positive effects, if the cannabis use is paired with a paleo diet.
Hi Katya,
ReplyDeleteWell, the thing is, PCOS like many modern diseases is multifaceted. There are multiple environmnental triggers and genetic predipositions, and not all cases of PCOS are the same. PCOS, like type II diabetes, actually is caused by many different kinds of genetic variations and environmental conditions.
I did not say PCOS women are unfit. I believe that most cases of PCOS are the result of genes which were once extremely evolutionarily adaptive. I believe many cases of PCOS are the result of genes evolutionarily selected for to help make a woman very good at becoming amenorrhetic in response to starvation. The REAL PURPOSE of PCOS genes is to make women good at developing hypothalamic amenorrhea in response to food deprivation. Hypothalamic amenorrhea is basically the inverse condition of PCOS - HA is a condition where the woman's brain stops making LH and FSH (as opposed to making too much), so that there is a functional inhibition of the ovaries. There are no follicles, therefore there are no cysts, because there are no brain hormones to tell the ovaries to do anything. The lack of LH and FSH in HA is from a lack of insulin, a lack of leptin (very specific), and an excess of cortisol (which is secondary to the lack of leptin, to some degree, as leptin inhibits the HPA axis).
Studies have shown that women HA, women who easily develop HA due to food restriction or stress, these women exhibit a PCOS-like response to overnutrition as well. It seems, then, that at least some cases of HA and some cases of PCOS are opposite conditions, with a similar genetic underpinning - nutrient state merely depends on which way you flip.
Overnutrition with glucose and fat? Multiple cystic follicles which did not rupture and anovulation thereby resulting. Undernutrition? No follicles, no ovarian function.
Speaking personally, I have PCOS, I was a classic case, almost primary amenorrhea (I had 1 cycle in my life with menstruation at 20 years old), LH:FSH ratio of 2:1, elevated androgens (testosterone, dheas) with symptomatic virulization (acne, hair growth), severe obesity (which was just as much a symptom as an exacerbating factor), signs of insulin excess like dark patches on my skin symptomatic of insulin hypertrophism (acanthosis nicgarans) and glucose disorders.
Then when I went on a low calorie, ketogenic diet, the PCOS went away. My LH:FSH level dropped and had a level of 1:1, I began having menstrual cycles every month, the acne disappeared and the hair growth stopped and lightened, the body fat melted off of me becuase my fat cells could no longer keep it in anymore (due to the decreased insulin, the fat poured out and made me nauseated if I tried to eat, and I had no appetite at all).
As I lost more and more weight, eventually I developed a new syndrome, hypothalamic amenorrhea. Symptomatically it is the exact inverse of PCOS. LH and FSH are low, but LH is very low and FSH is relatively higher (indicating a suppression of LH by cortisol and leptin deficiency). All gonadotropins are low, as are sex steroids. The problem this time is not dysfunctional ovulation with very high levels of gonadotropins and sex steroids, but a regression to an almost prepubertal state, the HPO axis is arrested, there is very low leptin, low FSH, even lower LH, low estrogen/testosterone.
And, in studies of women with HA, who easily develop HA, it is very common for them to have a vulnerability to PCOS if they are triggered with glucose disorders . My case is not that uncommon, the only thing which makes it uncommon is that it is very rare for a woman with PCOS to completely get control of the glucose problem, and weight, because food is plentiful in america and most women will not starve themselves. Because I am crazy, and starved myself for quite awhile, which got me down to a bit over 100 pounds. This then manifested my tendency to easily become hypothalmic amenorrhetic in response to food stress. (cont)
I know why I have PCOS. I seem to have inherited a trait(s) to have a very sensitive reproductive system from my maternal grandmother. My maternal grandmother was an immigrant from a recently modernized hunter gatherer tribe in north africa. Her mother, literally, LIVED IN A TRIBE. My great grandmother had tattoos all over her face and lived with a band of nomadic tribal people in north africa, and so did her ancestors.
ReplyDeleteIt would make perfect sense that my grandmother would have genetic traits which made her good at responding to starvation indicators, as her ancestors, recent ancestors, had a very unstable food supply and pregnancy while starving is FATAL. My grandmother was from a nomadic tribe... no fields of rice and wheat, its all the seasons and luck and weather.
My mother and grandmother all had fertility problems (late and irregular menstruation), although I am the only one with PCOS, and I know the only reason I have PCOS is because I was born into america in 1982, and drank corn syrup and ate foods that triggered what would otherwise be an adaptive evolutionary trait. If I did not drink kool aid at 11 by the pitcherful, I doubt I would have had such a problem with glucose disorder and thereby trigger PCOS.
So, personally, my experience and my research leads me to believe that PCOS is not really a "dysfunction", but it is an archaic trait which helped women predict and respond to starvation preemptively, by becoming infertile quickly/easily in response to stress and nutrient deprivaiton, thus increasing the chances of surviving famines. PCOS Is only what happens in 2011 when you grow up on diabetes-triggering foods which trigger the tendency to abnormal ovulation.
I believe that, perhaps, a high glucose intake may exhaust the woman with this trait's capacity to make inositol, and this is the triggering factor for PCOS. The low levels of inositol and specifically d-chiro-inositol just help inhibit ovarian function and ovulation in starvation, but when you pile on levels of sugar and carbohydrate and calories never before seen, the capacity to make inositol (to process insulin in insulin receptors) is overwhelmed easily, to the point where one develops an inositol deficiency not unlike someone taking depakote (depakote inhibits inositol synthesis, which then causes PCOS in women who otherwise would never have had it).
This trait - a tendency to easily disrupt ovulation and break the cycle - only causes PCOS in an environment like modern western society, where we eat food that causes glucose disorders from a grotesque amount of sugar and plant fats and calories, because the inositol making machinery are overwhelmed. This woud not be a condition in a natural environment where people are refeeding on normal food which is not grotesquely insulinotropic, which is NOT chemically engineered extremely calorie dense corn starch derived sugar.
If I were living in a north african tribe 200 years ago, my genes would only help me survive by not getting me knocked up when the food supply dropped off. My risk of PCOS would be nil, even during high calorie states, because a nomad in north africa will never see a chinese buffet, a pitcher of kool aid, or a giant bag of cheese doodles, or xtra large cups of ramen soup or any of the things that gave me PCOS but not my mother and not my grandmother (in spite of the fact they had late and irregular menstruation, they never had full PCOS with pathological symptoms and were fertile throughout their lives with many healthy live births and no miscarriages).
The other thing to consider with PCOS is that many women are misdiagnosed with PCOS when they actually have another condition. Its sorta a dumping ground diagnosis when a woman is fat (or blood sugar disorder), and has secondary amenorrhea, and some degree of virulization. But there are lots of things which cause this besides PCOS.
ReplyDeleteFor example, if you have the CAH trait, you will exhibit symptoms almost exactly like PCOS, but this is not PCOS because the dysfunction is in the adrenal glands and not the ovaries. The ovaries of a CAH woman are fine, the problem is that her enzyme to make cortisol is inefficient and low due to a single copy of a nonfunctional gene. This results in high levels of androgens being made (the precursor is androgenic) and the high levels of testosterone cause a secondary dysfunction in ovulation and virulization. The lab work will be very similar to PCOS, the main difference is that if she tests for the precursor to cortisol the levels will be very elevated whereas in PCOS it will be low and normal. It is important to be screened for CAH trait if you are a woman with PCOS because the treatment is completely different.
There are also many different TYPES of PCOS just as there are different types of type II diabetes. Some women with PCOS have pure ovarian origin of hormone excess; other women with PCOS have adrenal involvement (elevated DHEA-s), suggesting that subtle genetic atypicalities in adrenal gland enzymes may help trigger PCOS. There are maaaany different kinds of enzymes that control hormone synthesis from the adrenal glands, CAH is one of the most widely recognized dysfunctions there of... but a low grade enzyme insufficiency (or high activity in some cases) can result in a naturally high level of DHEA-S from the adrenal glands being made, which predisposes to PCOS by exacerbating dysfunctional ovulation.
Speaking personally, I suspect I have a genetic tendency to a high activity enzyme that makes DHEA-s. My PCOS involves high DHEA-s, and even when I had hypothalamic amenorrhea my DHEA-s was relatively high (it was not nearly as high as when I had PCOS, but it was a smidge above normal). I do not have CAH trait, so I suspect that I carry a genetic trait which makes my body efficient at making DHEA-s, probably a high activity enzyme or something. This alone did not cause PCOS, it just made it more severe and easily triggered.
About 50% of PCOS women have adrenal gland involvement, and these women are usually the ones with more severe symptomatic PCOS. It suggests that PCOS is not a disease with a single genetic cause, but a complex genetic-environment reaction, just like diabetes II. And like diabetes II, very rarely are two cases of PCOS the same.
I have totally regular normal menstruation with ovulation if I avoid high carbs, if I eat enough calories, if my leptin is adequate (via subcutaneous injections if the case need be), if I see bright light to stimulate the dopamine and norepinephrine and epinephrine require to trigger ovulation, if I do not have high stress, etc etc etc. I will ovulate every month, as if I had no endocrine disorder at all.
So, it suggests, that if I mimic my american lifestyle to replicate that of a north african nomad by seeing a lot of light and not eating a lot of carbs and not plowing myself with glucose but not starving either, then my reproductive system works just fine.
It makes a lot of sense why these genes would thrive in such a population. Amenorrhea saves lives when stress hormones rise, right? The environment these genes won in meant that stress indicated deprivation indicated death, and a hastier more certain one if a parasitic group of cells were rapidly multiplying in your uterus at the time of the deprivation.
Perhaps the reason a low dose of inositol works well for me is precisely because I have a mild "bipolar" vulnerability. If I, hypothetically, have a hyperkinetic second messenger system, it would take less inositol to have me less often in depression. Perhaps the patients who went manic on inositol just need a lower dose?
ReplyDeleteThen by the same token perhaps I would be wise to increase my inositol during depression.
...
Speaking more on the issue of syndromes/disease as indicating genetic "dysfunction"... I don't see it that way at all. Something may be genetically related which results in disease, but that does not mean the genes are dysfunctional.
Bipolar disorder, for example, a tendency to think faster and better and be more expansive and creative an active typically upon break of favorable weather, whereas in the unfavorable weather one falls into a torpor hibernation like state, can CLEARLY AND OBVIOUSLY be construed as an evolutionary advantage assuming the symptoms are not severe (e.g. you are not psychotic, you are not suicidal). Say you are a farmer, with what would today be called cyclothymia or bipolar II. It's march, the sun rises earlier, sets later, your brain speeds up and you have a ton of energy and motivation, and you get out to work before everyone else, and work hard, and grow a lot.
Then september comes and the opposite happens, you slow down, you feel down, you feel low, you don't want to do anything. The weather is now unfavorable, you hibernate, conserve energy.
The tendency for the brain to have this circadian rhythm boo-boo can actually be quite helpful in the right environment.
Cyclothymia and bipolar II are only a "disease" when you live in a modern society which expects routine clockwork behavior 9-5 living, with no highs, no lows, ever. Performance, consistently, every day, otherwise you are crazy. No, you are not allowed to take off 2 months from work due to depression, you are expected to come into work and be just as efficient as you were last june. If not, go to the psychiatrist and get that handled. or go on disability or whatever. Normal people work the same every all the time unless a situational life stress happens which sets them back.
AS for the classic and severe manic depression, bipolar I disorder, I tend to think this is the result of the aforementioned "bipolar genetic vulnerability" combining with brain-destroying environmental factors like severe omega 3 deficiency or severe stressors (which can and will rot the brain - schizophrenics, psychotic depressives, show similar brain degeneration and the root seems to be stress hormone mediated combined with a vulnerability to that).
Or infections prenatally which change genetics, or random genetic mutations, or what have you.
Cyclothymia and manic depression are not different diseases, they are the same disease, as in the same genes are involved. This is why cyclothymia is quite common in the families of manic depressives, indicating that cyclothymia is to manic depression what glucose intolerance is to severe type II diabetes. Not a different condition, its just that one is manifested in an extreme and pathological way.
I don't think genes for bipolar disorder are in of themselves "dysfunctional", they only turn out that way in the wrong time, the wrong century, the wrong profession, combined with the wrong lifestyle factors and experiences.
And, a lot of diseases are like that.
Genes for glucose intolerance (diabetes) are not dysfunctional. Genes for fat gain (obesity) are not dysfunctional. In 2011 america with a constant food supply, an excessive food supply, yes they are no longer adaptive and are now harmful, but the environment where these genes were selected they were useful.
Emily,
ReplyDeletei am a clinical herbalist, and wanted to share some thoughts about St John's Wort and its uses for depression.
when i think of St John's Wort, depression is the second thing that comes to mind -- liver health is the first. SJW has a powerful but fine action on the liver, increasing the pool of detox enzymes in the P450 pathway. this can speed up the rate at which it clears toxins from the blood -- which will include some pharmaceuticals. so we use care with it when someone is on a drug that is cleared through that pathway and has a touchy dose requirement -- things like HIV drugs, anti-rejection drugs after transplants, some heart medications, and (in some cases) artificial thyroid hormones. though it is often said that it will interfere with birth control pills, it is in my experience extremely unlikely that SJW alone could be responsible for rendering them ineffective; the dose of hormones in the pill is simply too high.
but the action that clears those drugs from the body is the same one that is beneficial in some types of depression. when the liver is overloaded with toxins (and here i'm referring more to buildup of endogenous metabolic waste products than to exogenous environmental toxins), the effects can cascade through the body, starting with impaired digestion, reduced nutrient absorption, and all the consequences of malnutrition. SJW and other herbs can clear that stagnation and so improve overall health, which includes mental health.
SJW is not hypericin. the whole plant is more effective than a standardized extract of a single constituent, as its natural balance of constituents has a synergistic effect on the action of the herb. it is also more effective when taken as tea than when dried and encapsulated. taken this way, it has its own actions on the serotonin receptors in the gut, but it also has a bitter flavor. (bitter herbs stimulate and coordinate digestive secretions and enzymes in the mouth, stomach, pancreas, liver, and intestines. taken before meals, they aid digestion.)
we think of SJW as definitively effective in depression rooted in liver stagnation or hormonal imbalance, but not so much when the depression is tied to a traumatic event or adrenal exhaustion. in those cases we work with other plants.
one other element i would add is that SJW would never be our sole recommendation for someone with depression, even if the type fit the criteria. dietary interventions to reduce NADs and get closer to an evolutionary diet, as well as activity, stress reduction, and sleep management strategies, are all part of the traditional herbalist's approach to any mental or physical illness.
regards,
ryn
I am bp and 4 me inositol is one of my wonder drugs. I take a tablespoon scoop in a glass of water approx 18 grams. I take it to control rage mania. It works well in 5 minutes. I get b12 injections as I have poor b12 uptake. Again I notice good things in a short time. I take a tabkespoon of the good mood altering blue ultraconcentrated omega3 to make my brain work in depression sometimes I double it with a chewable 5000mg b12. There are known genes for these issues. Li didn't do anything but make me feel sick. No rx 4 me thx. I enjoy going to the vitamin cottage instead. Online also good. No pills all liquids. Easy to adjust dose.
ReplyDeleteRead bipolar advantage. Bp is a symptom not a diagnosis per se like a cough. Some coughs are cancer some are TB some are a cold. Get your blood tested for vitamin D B12 copper zinc calcium only take things that make you feel stronger. Don't fear the mania or the depression. Fear is the mind killer (-:
Great to see you are interesting in alternative treatments for mental health. Are you aware of the research and work with Empower Micronutrients from Truehope and the work done by Bonnie Kaplan and Charles Popper?
ReplyDeleteLately the subject of B 12 has come up on some groups I am on at FB, enlightening actually. And considering also Folic acid apparently converted in the large intestines from B12??. Apparently has some function on mood.
ReplyDeleteAnd here this talk about b8, but b3 is also of interest, B3 is not actually a vitamin as I understand, but an amino acid, derived from tryptophan in the body?
And that this is helpful for depression and anxiety, as well as other disorders. Could you tie this together please, how these two work and what should be taken with them, and what the differences are? THNX
Great information, thank-you.
ReplyDeleteIs the half-life of inositol short enough that a bi-polar could supplement it only on down cycles?
I think phytate can quite possibly supply inositol if gut microbes like bifidus are able to dephosphorylate it.
ReplyDeletehttp://www.lucastafur.com/2011/10/is-phytate-really-problem.html
(If you haven't seen this blog, or recently, let me recommend it)
It is possible in the paleosphere may have misjudged phytate because it associates with known rascals.
My sister is suffering from Major depressive disorder and she is on effexor for last 1 month. I want to know if we can start giving her low doses of lecethin and inositol.any response will be truly appreciated.
ReplyDeleteWilliam Walsh (see his book Nutrient Power) uses inosital as part of a supplement package to treat depression, when the patient has low histamine levels in a blood test. The most important part of his treatment, when there is depression and low histamine, is folate/B12.
ReplyDeleteHe uses SAMe/methione to treat patients with high levels of histamine.
So I would expect controlled trials with inosital to show improvement in a subset of the patients; if the trial measured histamine and gave appropriate supplements as indicated (per Walsh), I would expect a much, much higher response rate.
Walsh's 'overmethylation' and 'undermethylation' recommendations are antiquated and too rigid. He still recommends folic acid for pete's sake...
DeleteI had a very distinct and interesting reaction to a daily dose of crystalline inositol, crystalline choline, and raw wheatgerm. The reaction was so strong, I had to convince myself not to be afraid of it. I was only 21 years old, so my interpretation of the effect was perhaps immature, but, at the time, I was certain that my ESP (yes, ExtraSensory Perception) had gone though the roof! I documented "incidents" in my journal.
ReplyDeleteThat was 30 years ago. The crystalline inositol became unavailable (when cocaine was a big deal) so I stopped taking the combo. (BTW, I'm not an illicit drug user, and never have been.) I've never experienced that remarkably strong feeling of ESP since, but I'll never forget it!
I used to be very "sensitive" as a child, often precognisant, but it has diminished as I aged (to my relief). I find your story interesting because an "event" just happened Sunday, the first in quite a while- 2 days after I started taking inositol powder. Even though I don't pursue this aspect of my personality I am curious as to the mechanism. Obviously ESP, gut feelings, women's intuition, and a person's 'sixth sense' come from some combination of physical, mental, emotional, possibly even spiritual states, and in that regard biochemistry makes the most sense to me.
Deleteok , I quit taking Lexapro as I had been taking it a while and its effectiveness was diminished . I purchased two lbs o inositol from Amaazon and just quit thr Lexapro after being on it for seven years . I had tapered down to 5 mg a day . I started with 12 gram of inositol per day . I had one day of moderate with drawl symptoms from the Lexapro .
ReplyDeleteCold hands , chills but that's all . About four days into this insomnia set in . I mean wide awake . I take a Lunesta which I hate doing but I need some sleep . Can inositol cause insomnia in this big dose ? Thanks
I struggle with depression every five years or so, and along with taking my antidepressant, I have added vitamins and minerals (after reading your blog). I purchaed a multivitamin (http://www.glutenfreevitamins.com/c-liac-vitality-multi-vitamin) but then realized that some of the minerals are an asparate/ascorbate complex. Is it a bad idea to take them if I am feeling depressed? I read George Eby's page about magnesium from aspartate being bad for depression. I really appreciate your blog! It helps me a lot, and beside, it's fascinating.
ReplyDeleteInositol ... I take it during the night... because it can make drowsy. I take about 10grams before going to bed and I sleep very good. I also take 5htp, glutamine and zma. During the day I take Alpha GPC, calcium supplement(with vitamin d, magnesium, zinc, copper) and some glutamine and I feel like the combination of these things made me very focused and raised my iq and reversed my aging. I look atleast 5 years younger after about 3 weeks on especially glutamine and alpha gpc. But good sleep will help also. Oh..btw..buying inositol powder is indeed much cheaper... I bought 500grams for about 50$.
ReplyDeleteWanted to share my experience w/ inositol. I've been battling w/ not too severe panic attacks/anxiety and mild depression for about 2 months now. It is not a normal thing for me, as I have only experienced this a few times in my life. I've been very proactive with exercise, getting more social interaction, joining a men's group, etc. I have not taking any medication, with the exception of 1/3 of a valium one night. I feel as though week-to-week I've been slowly improving. I ran into some info on inositol and then did a more thorough search on the internet. I was impressed that studies had shown it to be effective without severe side effects. I thought that inositol might be just the thing to help me break through the last stretch. I ordered some online and they arrived on Tuesday. I took one pill = 1g on Tuesday evening and experienced some anxiety that night. I took two pills on Wednesday (morning, afternoon) and had pretty bad anxiety that day. The type were everything was triggering it and every task I had to do felt overwhelming. I had not felt that type of anxiety during this bout. I took 3 pills on Thursday (spread out during the day) and had some anxiety Thursday morning, but the evening was okay. Then on Friday I took 2 pills (morning and at lunch). I was going to take 4, but the anxiety was awful. Probably my worst day since this all began 2 months ago. I stopped taking the inositol and by Friday evening I was feeling really good! Very relaxed and as good as I've felt in a while. Saturday I had one small panic attack in the morning but the afternoon was great. I had some anxiety Saturday evening and some today (Sunday), but nothing like I experienced Wednesday, Thursday morning, and Friday morning/afternoon. Right now things are feeling much more manageable. It's really hard for me to believe the inositol wasn't making my anxiety much worse. I just wanted to share my experience and see if others had a similar experience. I'm wondering if I should just take 1g/day for a couple weeks and see if that has any effect. My thinking was that my dosage was much smaller than the dosage used in the studies and I would work my way up daily and level out when I started feeling positive effects.
ReplyDeleteI was diagnosed as schizophrenic, but I also believe I'm bipolar too. I've been studying what causes my mood swings, and I thought I'd share a few thoughts with you. My mood swings are caused by a combination of the weather, caffeine use, and loud sudden noises. I've discovered reducing, or totally cutting out caffeine helps dramatically. Also, limiting light in sunny weather by wearing sunglasses prevents the anxious type 'high', and using a light box during the dark winter months eases the winter 'low'. Lecithin, or eating eggs regularly (which contain lecithin) also appears to help. Trying the inositol today, so will get back to you.
ReplyDeleteHere's my follow-up. Tried inositol, but it made my mood swings worse. I'm not saying don't take it, as a lot of people were helped by it, but be wary and carefully monitor whether your mood is flattening out or being made more unstable? I would recommend Yerba Mate tea for depression. It has a very low caffeine content if you choose the unsmoked version (don't have the smoked version, as it's been linked to various cancers due to the smoking in preparation), and has an anti-depressant effect.
ReplyDeleteI have been taking inositol for several years. When I was pregnant with my daughter, I had alternating bouts of unexplainable rage and very dark depression accompanied by suicidal thoughts. My midwife sent me for thyroid testing, which came back low. We treated the thyroid, which helped, but was not enough. We then added inositol to my regimen. I take it sublingually 1/4 tsp 3x a day. My results were dramatic. It was as if a dark mantle lifted from my shoulders. I have continued on it successfully for some time now. Although, I still suffer from PMS in a debilitating way UNLESS I remain on Krill Oil daily. I struggled with low energy for years, and B12, also sublingual, is helpful in this area. One strange phenomenon: if I take Calcium supplements, I am like a zombie. I can hardly wake up and go through the day in a fog. Could the inositol be causing this strange interaction?
ReplyDeleteI came across this blog while researching inositol as an ingredient in a sleep supplement I purchased at a chiropractic office. The supplement also included Melatonin, B6 and L-theanine and I was trying to determine if it was safe to use with a blood thinner and a beta blocker. The blog was very helpful in understanding what inositol is and does, thank you for that. In reading through some of the other comments regarding Krill Oil and it's usefulness as an anti-inflammatory I envy those who can use it. Because of it's blood thinning properties as well I cannot use it since being put on a prescription blood thinner for A-fib. Due to neck, shoulder and hip pain from old injuries I have been on a quest to find something that works for pain/inflammation that can safely be used with blood thinners- so far not much luck-any suggestions?
ReplyDeleteI'm 17 years old and this crap is amazing. I've been though pill after pill after therapy. And let me just say this crap works. I'm 17 by the way so i say crap a lot. I'm a free soul again. You should take it. I wish you luck. Live long and prosper.
ReplyDeleteSorry if someone already brought this up ( I didn't read all the comments) Inositol also has an application for reducing the psoriasis that can be induced by lithium. The effects lithium has on the gut lining and the support inositol gives to cell membrane integrity may offer additional clues to its mechanism of benefit.
ReplyDeleteI want to add my experience with inositol which has been very helpful for me. I have genetic mutations that cause mental illness. Right now I am on Lmethylfolate and will be finding out more about my chromosomes soon. But the point is I have longed suffered from depression. Both my mom and grandma where institutionalized.
ReplyDeleteI have been diagnosed as bipolar, PTSD and most recently major depressive disorder and ADD. I am now off all pharmaceuticals except gabapentin for sleep.
Along with my depression, I have long had terrible anxiety. When my psych who is sort of wholisitic, put me on inositol, my anxiety disappeared immediately and my moods are much more stable and "soft". I take a very high dose: 16 mg. a day. And I am fine with that. There is evidence on the web for this dosage and my doc is very evidence based.
One weird thing that has happened is that BEFORE I took the inositol I discovered how good tyrosine made me feel. My doc says he doesn't like tyrosine, I think he considers it activating for bipolar. But get this: he had me try ritalin! Now that made me totally nuts. I never felt so much rage.
But back to my concern. When I began the inositol, the tyrosine stopped working, at least sort of. Any ideas why that would happen?
Thanks. Nice to find this blog.