It is no secret that on this blog, I am a reductionist. All psychiatric illness (shoot, all of chronic Western disease) has the same pathology (inflammation) and starts with the same treatment (an anti-inflammatory lifestyle, including diet, healthy coping and stress amelioration, and good sleep).
At an individual level, of course, it is not so simple. I can't be an effective doctor for you without knowing your experience, and spending enough time with you to figure out how you tick. That way I can modulate my advice to meet you where you are. And that in a nutshell is the failing of modern medicine. It tries to replace a personal relationship with testing and algorithms in the name of science, efficiency, and expediency. Problem is, for a doctor (especially a primary care doctor), such a practice is soul-killing (who wants to be responsible, in a litigious society especially, for the health of 5000 patients you barely know?). For the nation, the algorithm is expensive, careless, and dangerous. It works for the protoypical patient and in some obvious areas, such as safety checklists and counts in the operating room, but once anyone comes in with human quirks and complications, the data goes out the window. Not to mention the ridiculous attention to relatively meaningless numbers (cholesterol panels, for example) in lieu of a rational human-friendly evolutionary model for health.
I live in Massachusetts, where managed care has a prominent role. In psychiatry, several insurance companies have attempted to gather data based on various scales and standardize treatment to some extent. I've participated (somewhat unwillingly - as it was clear from the outset the data gathering would simply use valuable time and resources better directed towards other things) in these endeavors, and also in research. In the "real world" the use of scales to try to gather data for what works for the insurance company has proven each time to be a complicated disaster, and has been abandoned. People in my waiting room aren't particularly interested in filling out the scales the insurance company wants them to, and thus the results are conflicting and meaningless. In research or in the symptom scale measures I might choose for my patients based on our relationship and my knowledge of their history, there is a different sort of vibe. It's a collaboration. It's personalized medicine. In research, the patients are pre-selected not to have certain comorbidities (so in general they are less complicated than the patients who show up at the actual doctor's office), and they are volunteers, even paid volunteers!
With enough data points and a big enough computer, I'm sure more rational models of algorithm care could be produced. But for now, nothing replaces simply knowing your patient and spending time learning who they are. Nothing replaces the art of medicine, particularly, I think, the art of personalized psychiatry. And, perhaps counter-intuitively, we all suffer when medicine becomes increasingly compartmentalized and specialized. All doctors should be generalists and have a robust clinical knowledge of all fields. Recently, my consultations have been instrumental in diagnosing two cases of hyperparathyroidism - the only reason it came down to me is that I am the only one in a managed care model who has more than about 5 minutes at a time to spend with patients. I'm expensive (being extensively, expertly trained over many, many years), but I like to think I'm worth it. That said, your psychiatrist should not be diagnosing your hyperparathyroidism. That's a travesty and a failure of modern medicine.
But - we stand to learn a great deal and develop confidence and wisdom if we dial down on the specific pathophysiology and genetics of psychiatric disorders. And what we find, more and more (which is what one would suspect, from the Grand Unified Inflammation Theory), is that the pathologies and genetics overlap. Another Nature paper came out recently, sent to me by Jamie Scott, that brings together the disparate diseases of schizophrenia and anxiety. And that's kinda cool. Let's break it down.
Convergent functional genomics of anxiety disorder: translational identification of genes, biomarkers, pathways, and mechanisms
A bit about anxiety. It is the most prevalent psychiatric disorder, affecting 18.1% of Americans annually, but remarkably enough, less studied in a rigorous sense than the much more rare schizophrenia or autism spectrum disorders. Some anxiety disorders seem to be based on an anxious temperament (generalized anxiety disorder, panic disorder) whereas others are based on obvious stressors (phobias, PTSD). Others are mixed, like obsessive compulsive disorder. Anxiety is typically along for the ride in depression (at least in the patients I see), and makes for a more complex patient more resistant to typical treatment. In general, anxiety can be defined as a pathologic increased reactivity to the environment, driven by fear and uncertainty in light of perceived threats.
Anxiety disorders are the protoypical disorder of the modern world, where our hunter-gatherer brains are trying to manage remembering 50 passwords, the threat of H1N1 and terrorism, kidnapping and car accidents.
In the Nature paper, the authors used human and animal genetic data (emphasizing the gene expression studies rather than the specific gene studies) plus some controlled animal trials to dig up the most likely genes that might give you a predisposition to be more anxious than usual. Not surprisingly, they found a lot of genes that were active in the hippocampus, related to stress hormone response and GABA transmission. Other genes, such as polymorphisms in the dopamine system, are also obvious, and the "grand unified theory" supporting evidence is that many of these genes are also suspected to be awry in bipolar disorder, schizophrenia, and depressive disorders. One suspect gene (QKI) has a central role in myelination, is a biomarker for anxiety, and there is evidence of changes in the expression in humans of QK1 in response to stress.
One of the top genetic pathways suspected in anxiety is also the pathway associated with signaling in Huntington's disease - a disease that is (speculatively) perhaps strongly associated with wheat consumption. Gene expression, again, has been emphasized, which accounts for genetics, epigenetics, and environmental regulation. "Genes that change together act together" - "the co-expression data sets… generted in various brain regions offer testable hypothesis for transcriptional co-regulation, and for epistatic interactions among the corresponding loci."
In English? Our genes code our vulnerability to environmental insult. Some of the same genes that make you vulnerable to schizophrenia also make you vulnerable to anxiety and depression. The environmental insult is typically modulated through the stress response system, which is also modulated through diet and experience and movement and sleep.
Live and move and work and think like a human, and you will be more resilient. Stray from our evolutionary programming, and you are going out on a limb.
Sunday, May 29, 2011
Friday, May 27, 2011
New Studies: Nutritional and Pathologic Clues in Autism
I've devoted quite a few entires to autism (more properly called the autism spectrum disorders). Perhaps because the illness can be so devastating, attacks so young, and is so mysterious in its origin. I've migrated many of the autism entries over to Psychology Today, and the specifically nutritionally-related ones can be found here:
Diet and Autism
Diet and Autism - Newer Studies and Intriguing Links
Autism, Inflammation, Speculation, and Nutrition
The first new paper I want to present today is a Letter in Nature: Transcriptomic analysis of autistic brain reveals convergent molecular pathology. Like most Nature papers, the prose is dense with advanced molecular biology and neuroscience, but I think I can glean the meaning of it. In this study, the researchers examined post-mortem brains from 19 autism cases and 17 controls. They focused on three areas previously shown to be different in the autistic brain (specifically areas of the cerebral cortex and cerebellum), finding the most differences between autistic brains and controls in the cortex.
What is interesting about these sorts of studies is that they look at gene expression rather than just genetics, meaning they find out which genes are activated differently between cases and controls. They found that many different genes were affected (consistent with the findings in autism in general - there is no single "autism gene" causing all cases, though 1% of cases have a 15q duplication, for example). The interesting part is that the gene expression that was different between cases and controls clustered around specific areas, and were highly related to what is called "cortical patterning." These are some of the same gene areas that were already suspected to be causative for autism spectrum disorders, and are also suspected to be causative in schizophrenia. Other genes that were upregulated were functioning as part of the immune and inflammatory response.
What is intriguing about this study is that the researchers felt it showed convergence of the many different genetic causes in the area of transcription and splicing of certain genes as the underlying mechanism of the disorder. They were also able to show that the inflammation was secondary rather than primary.
All right, we made it through the tough part. Now on to the second paper, which is far more nutritionally related (possibly - it's just an observational study, but it is interesting). Prenatal Vitamins, One-carbon Metabolism Gene Variants and Risk for Autism.
So, the intro - Prevalence in the US is about 1 in 110 children and may be rising (a recent Yale study in South Korea study suggests autism affects 1 in 38 children there). It is widely accepted that genetic risk underlies the disorder, but there are also definitely interactions with environmental factors. The recent study showing increased risk of autism in short intervals between pregnancies could implicate nutritional factors. Valproic Acid (depakote) which disrupts folate metabolism is a known cause of autism and neural tube defects.
Other literature suggest that some children with autism have altered B vitamin metabolism and a reduced ability to methylate things. So in this brand new study, the researchers specifically looked at vitamin supplement intake. Children with autism in California were identified as part of large, population-based, case-control CHARGE study. Their mothers were asked in telephone interviews whether they consumed prenatal vitamins, multivitamins, fortified cereals, and other supplements in the period 3 months before conception, and then during pregnancy and breastfeeding. If they answered yes, they were asked specifically what vitamins and brands were consumed.
Interesting results ensued - 97% of mothers of the normal controls and 96% of mothers of the children with autism reported taking prenatal vitamins. However, mothers who took the vitamins in the 3 months before conception and in the first month of pregnancy were significantly less likely to have autistic children than those who didn't. There was no difference between vitamin and non-vitamin takers in months 2-9 of pregnancy or later. The findings were controlled for various confounders, such as mom's education, race, whether conception was intentional or not, year of birth, etc.
Even more interesting - use of regular multivitamins in lieu of the prenatals was not associated with decreased risk of autism compared to taking no vitamins. The major difference between most prenatal vitamins and regular multis is a doubling of folic acid. The government says the synthetic folic acid is the same as the folate in food - Chris Kresser notes here that conversion from synthetic folic acid to the active tetrahydrofolate is poor in humans, and while synthetic folic acid pretty definitely reduces risk of neural tube defects, it also likely increases the risk of cancer - these kinds of population risks are a tough call. If you are trying to get pregnant and you aren't always sure you are getting a lot of folate from foods, it may well be worth the risk to take synthetic folic acid for the periconception period. Well, that's something to chew on.
The researchers in this study also checked genetics, finding that children with methylation issues (related to the folate cycle) were also more likely to have autism. Maternal periconceptual folic acid seems to increase methylation in specific gene regions in the child (1), which can have epigenetic effects that can affect a child throughout life.
Get nutrients from food whenever possible, but there are certain circumstances in which wise supplementation may be very important. And for public health recommendations (assuming the SAD) - supplementation for women trying to become pregnant seems wise, and when one reviews IOM and other reports, one often sees a fair accounting of the risks involved. In fact, that is often why IOM or other recommendations seem quite conservative. The questions continue!
Diet and Autism
Diet and Autism - Newer Studies and Intriguing Links
Autism, Inflammation, Speculation, and Nutrition
The first new paper I want to present today is a Letter in Nature: Transcriptomic analysis of autistic brain reveals convergent molecular pathology. Like most Nature papers, the prose is dense with advanced molecular biology and neuroscience, but I think I can glean the meaning of it. In this study, the researchers examined post-mortem brains from 19 autism cases and 17 controls. They focused on three areas previously shown to be different in the autistic brain (specifically areas of the cerebral cortex and cerebellum), finding the most differences between autistic brains and controls in the cortex.
What is interesting about these sorts of studies is that they look at gene expression rather than just genetics, meaning they find out which genes are activated differently between cases and controls. They found that many different genes were affected (consistent with the findings in autism in general - there is no single "autism gene" causing all cases, though 1% of cases have a 15q duplication, for example). The interesting part is that the gene expression that was different between cases and controls clustered around specific areas, and were highly related to what is called "cortical patterning." These are some of the same gene areas that were already suspected to be causative for autism spectrum disorders, and are also suspected to be causative in schizophrenia. Other genes that were upregulated were functioning as part of the immune and inflammatory response.
What is intriguing about this study is that the researchers felt it showed convergence of the many different genetic causes in the area of transcription and splicing of certain genes as the underlying mechanism of the disorder. They were also able to show that the inflammation was secondary rather than primary.
All right, we made it through the tough part. Now on to the second paper, which is far more nutritionally related (possibly - it's just an observational study, but it is interesting). Prenatal Vitamins, One-carbon Metabolism Gene Variants and Risk for Autism.
So, the intro - Prevalence in the US is about 1 in 110 children and may be rising (a recent Yale study in South Korea study suggests autism affects 1 in 38 children there). It is widely accepted that genetic risk underlies the disorder, but there are also definitely interactions with environmental factors. The recent study showing increased risk of autism in short intervals between pregnancies could implicate nutritional factors. Valproic Acid (depakote) which disrupts folate metabolism is a known cause of autism and neural tube defects.
Other literature suggest that some children with autism have altered B vitamin metabolism and a reduced ability to methylate things. So in this brand new study, the researchers specifically looked at vitamin supplement intake. Children with autism in California were identified as part of large, population-based, case-control CHARGE study. Their mothers were asked in telephone interviews whether they consumed prenatal vitamins, multivitamins, fortified cereals, and other supplements in the period 3 months before conception, and then during pregnancy and breastfeeding. If they answered yes, they were asked specifically what vitamins and brands were consumed.
Interesting results ensued - 97% of mothers of the normal controls and 96% of mothers of the children with autism reported taking prenatal vitamins. However, mothers who took the vitamins in the 3 months before conception and in the first month of pregnancy were significantly less likely to have autistic children than those who didn't. There was no difference between vitamin and non-vitamin takers in months 2-9 of pregnancy or later. The findings were controlled for various confounders, such as mom's education, race, whether conception was intentional or not, year of birth, etc.
Even more interesting - use of regular multivitamins in lieu of the prenatals was not associated with decreased risk of autism compared to taking no vitamins. The major difference between most prenatal vitamins and regular multis is a doubling of folic acid. The government says the synthetic folic acid is the same as the folate in food - Chris Kresser notes here that conversion from synthetic folic acid to the active tetrahydrofolate is poor in humans, and while synthetic folic acid pretty definitely reduces risk of neural tube defects, it also likely increases the risk of cancer - these kinds of population risks are a tough call. If you are trying to get pregnant and you aren't always sure you are getting a lot of folate from foods, it may well be worth the risk to take synthetic folic acid for the periconception period. Well, that's something to chew on.
The researchers in this study also checked genetics, finding that children with methylation issues (related to the folate cycle) were also more likely to have autism. Maternal periconceptual folic acid seems to increase methylation in specific gene regions in the child (1), which can have epigenetic effects that can affect a child throughout life.
Get nutrients from food whenever possible, but there are certain circumstances in which wise supplementation may be very important. And for public health recommendations (assuming the SAD) - supplementation for women trying to become pregnant seems wise, and when one reviews IOM and other reports, one often sees a fair accounting of the risks involved. In fact, that is often why IOM or other recommendations seem quite conservative. The questions continue!
Tuesday, May 24, 2011
More Exciting News
Yesterday I received an email from Brent Pottenger offering up an open spot as a presenter at the Ancestral Health Symposium in a couple of months. Since I'm already going and I've already booked the accommodations, seems like a no-brainer to accept the invitation - also, I get to present with Jamie Scott, so double bonus! We will do something along the lines of evolutionary medicine as a model for resiliency of body and mind, or maybe Forging Superhumans with Coconut Butter. We'll have to see what unfolds.
The bummer part is that it looks like we will be presenting at the same time as Stephan Guyenet, and I was really looking forward to his talk! Oh well - the 16 of you who stay in our room for our presentation are hopefully in for some fun times.
In other news, I updated my Fructose Malabsorption and Depression post for Psychology Today (now called Could Soda and Sugar Be Causing Your Depression?) including some extra studies. That one could be important - and it would be nice if you clicked over there, stumbleupon and retweet so that maybe someone with a nose and budget for research will really look into it.
New posts later this week!
The bummer part is that it looks like we will be presenting at the same time as Stephan Guyenet, and I was really looking forward to his talk! Oh well - the 16 of you who stay in our room for our presentation are hopefully in for some fun times.
In other news, I updated my Fructose Malabsorption and Depression post for Psychology Today (now called Could Soda and Sugar Be Causing Your Depression?) including some extra studies. That one could be important - and it would be nice if you clicked over there, stumbleupon and retweet so that maybe someone with a nose and budget for research will really look into it.
New posts later this week!
Monday, May 23, 2011
A Testimonial
Posted over at Robb Wolf's site with a commentary by Mat Lalonde - a child with significant improvement in autism symptoms mere days initiating a casein free, gluten-free paleo diet:
Scarlet's turnaround
- Posted using BlogPress from my iPhone
Scarlet's turnaround
- Posted using BlogPress from my iPhone
Friday, May 20, 2011
More About the Mysteries of Cannabis
In my last post on cannabis, I reviewed some observational evidence that smoking marijuana could be seriously bad news if you have psychosis or relatives who do, putting you at higher risk for psychosis yourself. Ultimately there will be no gold standard randomized controlled trial - the design for that would be: randomize one group of teenagers at high risk for psychosis to smoking pot (hey, make it multi-arm - some will smoke LOTS of pot, and others less), and have another group not smoke pot, follow them through young adulthood, and see what happens.
Yeah, that's not going to happen. But what we do have as evidence in several epidemiologic studies and some prospective cohort trials is that the more pot and the earlier a teenager starts smoking pot, the higher the risk of developing psychosis. We also have some plausible biologic mechanisms (this study, for example, seems to show that folks with cannabis dependence and folks with schizophrenia have similar brain metabolism in key areas, which were significantly different than non-schizophrenic non-cannabis dependent folks). And in animal studies, where randomized controlled trials can be done, heavy doses of THC seemed to damage the brain.
I feel like music. How about Austin's own Spoon, with Don't You Evah (right click to open in new tab).
Is the news all bad for funny cigarettes? Any time one badmouths marijuana or questions its benefits one will find that a bunch of people pop up with all sorts of miraculous properties of cannabis. And, in truth, cannabis is not just about THC, and is an exceedingly interesting plant with all sorts of intriguing cannabinoids in it. As commenter Erik noted, cannabidiol seems to be neuroprotective and balance some of the more toxic effects of THC, suggesting that "vintage pot" with a better ratio between the two might be much healthier.
I have used cannabinoids clinically (never in psychiatry, however) - there is an FDA-approved synthetic THC called marinol that we used to give out on the cancer ward in medical school, in Texas, to cachectic patients who had no appetite. Back then before the proliferation of a ton of antiretrovirals we saw a lot more advanced AIDS - those patients also seemed to benefit from marinol to increase appetite. I must say I did a number of consults on hospitalized cancer patients in Massachusetts, but never saw marinol prescribed up here. If you look at the link to marinol you will find the DEA page describing that the purified synthetic THC is much safer than cannabis smoked au naturale.
Some of the DEA's points are valid - lord knows what is in the cannabis you might buy from your friendly neighborhood dealer - and certainly in the case of immunosuppressed cancer and advanced AIDS patients, smoked joints could easily be adulterated with natural fungi that grow into big nasty (and deadly) fungus balls in the lung. I saw a case of this fungus ball in medical school in a patient immunosuppresed with HIV who also happened to smoke a lot of pot. It could have been from other sources, of course, but my attendings assured me they had seen it several times in AIDS patients who were heavy pot users. It's not a pleasant way to go, and the treatments are horrible.
(Over time, you see enough cognitively bereft heavy pot users and psychotic heavy pot users and top that off with deadly fungus balls, and you can see why I'm none too fond of the stuff. These types of experiences are anecdotal, but influential to any doctor in practice. Part of being human, I suppose.)
Other DEA points are the same old conventional wisdom and faulty reasoning that led T. Colin Campbell to conclude that animal protein causes cancer from some rodent studies using isolated casein and aflatoxin. Natural cannabis contains a mixture of cannabinoids with different effects - one can't necessarily extrapolate the effects of just THC to marijuana in general (though it seems more reasonable to do so with the modern "skunk" high-THC marijuana). And "purified synthetic THC" could be kinda like casein without the whey in aflatoxin-poisoned rodents - a bad idea for pretty much anyone if you aren't a step away from death via advanced disease + starvation.
So, the lengthy intro aside, let's examine some of the evidence for marijuana that shows positive effects in the human brain. Fortunately we have the Rolls Royce of academic reviews available - a Cochrane Review - Cannabinoids for the treatment of dementia.
So what's the good news for marijuana? Well, cannabis receptor 1 and 2 (CB1 and CB2). CB1 is primarily active in the central nervous system, and CB2 is found more in the periphery, particularly on the white blood cells. Some studies of cannabinoids seem to find them to be, in the whole, neuroprotective. They regulate glutamate transmission (reducing neurotoxicity) and may reduce neuroinflammation. They might protect the brain from toxic injury. THC may also be what is called a cholinesterase inhibitor, which is a class of drugs that are now used to treat Alzheimer's.
Small open label trials showed that marinol (synthetic THC) reduced agitation and helped weight gain in dementia patients. Another small trial of cannabidiol showed it helped with sleep. But, as Peter has been known to say, small, third-rate studies are small, third-rate studies, and do little more than give us a reason to design larger, better studies that might prove a point or two. The great thing about a Cochrane review is those scientists comb MEDLINE and OVID and conference reports and ongoing research trials and PUBMED for the awesome studies. Those that are randomized, controlled, and done with acceptable follow-up and inclusion criteria. And when you comb the literature for that sort of study with respect to cannabis products and dementia, you find one study that wasn't even the greatest of studies (15 patients, using marinol), so the reviewers ultimately have to say there is no reliable evidence that cannabis should be used clinically in dementia patients.
And what about non-dementia, non-psychosis studies - neuroimaging studies, for example? After all, I treat a particular population - one apt to be anxious, depressed, demented, or psychotic. If you are none of the above, are not at high risk for psychosis (ie no family members with psychotic disorders and no personal history), and like to spend the days smoking out on your mom's basement couch - how risky is it to your brain? Well, a neuroimaging review seems to indicate there are metabolic changes in the brain related to smoking pot, but no one is sure what it means. Other kinds of studies of neuropsychologic testing also show mixed results.
What seems to be the consensus when one reads general articles meant for psychiatrists (in Psychiatric Times, for example), is that marijuana in the brain is perhaps best conceptualized as a potent nerve growth factor. In a young, growing brain (a teenager), likely replete with plenty of nerve growth factor, extra nerve growth factor has the potential to be disastrous - lighter fluid on a briskly burning fire. In an older, demented brain (a smoldering, dying fire), nerve growth factor may well be therapeutic, but there isn't enough good evidence to conclude that is the case.
Is marijuana "paleo?" The anthropologists can answer that question far better than I can. Is it healthy? I can name circumstances which encompass the majority of my patients in which there is some reasonable evidence that it is most likely very unhealthy and risky. I'm willing to withhold judgment about it's ultimate therapeutic value in other cases (like dementia) until more evidence is in. And certainly there will, logically, be a difference between artisan variety vintage stuff than the "skunk" high-THC brands of today.
And let's not forget the underlying evolutionary principle - human babies born of natural eating and natural living mothers and fathers are strong and amazing and not broken. We are not automobiles - when left to an evolutionary diet and activities we are likely to thrive, as we always have. And cannabis has the potential to be a potent long-term brain-altering substance. There's an old adage in psychiatry: Don't fix what ain't broken.
In the modern world, well, let's hope the science researchers design and implement some good studies that can answer our questions!
Yeah, that's not going to happen. But what we do have as evidence in several epidemiologic studies and some prospective cohort trials is that the more pot and the earlier a teenager starts smoking pot, the higher the risk of developing psychosis. We also have some plausible biologic mechanisms (this study, for example, seems to show that folks with cannabis dependence and folks with schizophrenia have similar brain metabolism in key areas, which were significantly different than non-schizophrenic non-cannabis dependent folks). And in animal studies, where randomized controlled trials can be done, heavy doses of THC seemed to damage the brain.
I feel like music. How about Austin's own Spoon, with Don't You Evah (right click to open in new tab).
Is the news all bad for funny cigarettes? Any time one badmouths marijuana or questions its benefits one will find that a bunch of people pop up with all sorts of miraculous properties of cannabis. And, in truth, cannabis is not just about THC, and is an exceedingly interesting plant with all sorts of intriguing cannabinoids in it. As commenter Erik noted, cannabidiol seems to be neuroprotective and balance some of the more toxic effects of THC, suggesting that "vintage pot" with a better ratio between the two might be much healthier.
I have used cannabinoids clinically (never in psychiatry, however) - there is an FDA-approved synthetic THC called marinol that we used to give out on the cancer ward in medical school, in Texas, to cachectic patients who had no appetite. Back then before the proliferation of a ton of antiretrovirals we saw a lot more advanced AIDS - those patients also seemed to benefit from marinol to increase appetite. I must say I did a number of consults on hospitalized cancer patients in Massachusetts, but never saw marinol prescribed up here. If you look at the link to marinol you will find the DEA page describing that the purified synthetic THC is much safer than cannabis smoked au naturale.
Some of the DEA's points are valid - lord knows what is in the cannabis you might buy from your friendly neighborhood dealer - and certainly in the case of immunosuppressed cancer and advanced AIDS patients, smoked joints could easily be adulterated with natural fungi that grow into big nasty (and deadly) fungus balls in the lung. I saw a case of this fungus ball in medical school in a patient immunosuppresed with HIV who also happened to smoke a lot of pot. It could have been from other sources, of course, but my attendings assured me they had seen it several times in AIDS patients who were heavy pot users. It's not a pleasant way to go, and the treatments are horrible.
(Over time, you see enough cognitively bereft heavy pot users and psychotic heavy pot users and top that off with deadly fungus balls, and you can see why I'm none too fond of the stuff. These types of experiences are anecdotal, but influential to any doctor in practice. Part of being human, I suppose.)
Other DEA points are the same old conventional wisdom and faulty reasoning that led T. Colin Campbell to conclude that animal protein causes cancer from some rodent studies using isolated casein and aflatoxin. Natural cannabis contains a mixture of cannabinoids with different effects - one can't necessarily extrapolate the effects of just THC to marijuana in general (though it seems more reasonable to do so with the modern "skunk" high-THC marijuana). And "purified synthetic THC" could be kinda like casein without the whey in aflatoxin-poisoned rodents - a bad idea for pretty much anyone if you aren't a step away from death via advanced disease + starvation.
So, the lengthy intro aside, let's examine some of the evidence for marijuana that shows positive effects in the human brain. Fortunately we have the Rolls Royce of academic reviews available - a Cochrane Review - Cannabinoids for the treatment of dementia.
So what's the good news for marijuana? Well, cannabis receptor 1 and 2 (CB1 and CB2). CB1 is primarily active in the central nervous system, and CB2 is found more in the periphery, particularly on the white blood cells. Some studies of cannabinoids seem to find them to be, in the whole, neuroprotective. They regulate glutamate transmission (reducing neurotoxicity) and may reduce neuroinflammation. They might protect the brain from toxic injury. THC may also be what is called a cholinesterase inhibitor, which is a class of drugs that are now used to treat Alzheimer's.
Small open label trials showed that marinol (synthetic THC) reduced agitation and helped weight gain in dementia patients. Another small trial of cannabidiol showed it helped with sleep. But, as Peter has been known to say, small, third-rate studies are small, third-rate studies, and do little more than give us a reason to design larger, better studies that might prove a point or two. The great thing about a Cochrane review is those scientists comb MEDLINE and OVID and conference reports and ongoing research trials and PUBMED for the awesome studies. Those that are randomized, controlled, and done with acceptable follow-up and inclusion criteria. And when you comb the literature for that sort of study with respect to cannabis products and dementia, you find one study that wasn't even the greatest of studies (15 patients, using marinol), so the reviewers ultimately have to say there is no reliable evidence that cannabis should be used clinically in dementia patients.
And what about non-dementia, non-psychosis studies - neuroimaging studies, for example? After all, I treat a particular population - one apt to be anxious, depressed, demented, or psychotic. If you are none of the above, are not at high risk for psychosis (ie no family members with psychotic disorders and no personal history), and like to spend the days smoking out on your mom's basement couch - how risky is it to your brain? Well, a neuroimaging review seems to indicate there are metabolic changes in the brain related to smoking pot, but no one is sure what it means. Other kinds of studies of neuropsychologic testing also show mixed results.
What seems to be the consensus when one reads general articles meant for psychiatrists (in Psychiatric Times, for example), is that marijuana in the brain is perhaps best conceptualized as a potent nerve growth factor. In a young, growing brain (a teenager), likely replete with plenty of nerve growth factor, extra nerve growth factor has the potential to be disastrous - lighter fluid on a briskly burning fire. In an older, demented brain (a smoldering, dying fire), nerve growth factor may well be therapeutic, but there isn't enough good evidence to conclude that is the case.
Is marijuana "paleo?" The anthropologists can answer that question far better than I can. Is it healthy? I can name circumstances which encompass the majority of my patients in which there is some reasonable evidence that it is most likely very unhealthy and risky. I'm willing to withhold judgment about it's ultimate therapeutic value in other cases (like dementia) until more evidence is in. And certainly there will, logically, be a difference between artisan variety vintage stuff than the "skunk" high-THC brands of today.
And let's not forget the underlying evolutionary principle - human babies born of natural eating and natural living mothers and fathers are strong and amazing and not broken. We are not automobiles - when left to an evolutionary diet and activities we are likely to thrive, as we always have. And cannabis has the potential to be a potent long-term brain-altering substance. There's an old adage in psychiatry: Don't fix what ain't broken.
In the modern world, well, let's hope the science researchers design and implement some good studies that can answer our questions!
Tuesday, May 17, 2011
Dopamine Series at Psychology Today
Dopamine Primer
Dopamine, the Left Brain, Women, and Men
Genius and Madness
Dopamine, the Left Brain, Women, and Men
Genius and Madness
Sunday, May 15, 2011
Cannabis and Psychosis
One of the best things about my blogging gig over at Psychology Today is that I've now attracted the attention of more researchers in the field from all over the world. I'm a clinician doing my work in a suburb of Boston - I know some pretty cool and important people who make amazing research contributions, but I am certainly not among them. Most of my musings here at Evolutionary Psychiatry are theoretical - there are NO paleo 2.0 diet trials for any psychiatric condition, after all. If someone walks into my clinic with bipolar disorder, I can't say "oh, just try a ketogenic diet and a multimineral and you will be fine." There are no trials and case studies of ketogenic diets in the literature were failures.
That doesn't mean I don't push for elimination of food toxins, put in a little plug for pasture butter, demonstrate and encourage stress reduction techniques, focus on good sleep hygiene (and look for sleep disturbance and medical causes), and I do take people off statins when there is good clinical reason (primarily in folks with dementia, with good results, actually. Also, a couple of cases of resistant depression.) But I can't go full-blown evolutionary psychiatry with all my patients. Some aren't interested, and for others the data isn't there. Which is okay. EvPsych has reinvigorated my interest in the field and in research, and I feel the preventative potential of a paleo 2.0 diet is amazing - so for subclinical disease, I feel my blog and the diet are likely doing a lot of good, far more good than I could do in the time I have to see patients one by one. But I don't have any proof of that. Which is okay. I'll still keep looking for more evidence and more nutritional links.
But! Cannabis! I am honored that my twitter feed (warning - I might tweet about Crossfit, shampoo, and my children) is followed by Dr. Sanjuan in Spain, who sent me a link to this article, which among other articles will be the anchor for this post.
Cannabis. Evo Med is the province of rebels, and rebels love pot...
Pot might not love you.
Cannabis is the world's most popular recreational drug and its use has accelerated among adolescents in the United States.
There are two circumstances in which I tend to see heavy pot use - young people struggling with psychotic disorders, and older folks with lifetime heavy pot use struggling with cognitive function and anxiety problems. Such circumstances are weighted to bias my opinion against pot as the happy self-medication of choice. You are forewarned!
Cannabis use has a high comorbidity with populations with psychotic disorders. Its continued use is associated with poor outcomes in psychosis and with more frequent and earlier relapses (1). Use has been associated as a risk factor for emerging psychosis, and a young person with heavy use will have a two-fold risk of developing psychosis (2)(3). The earlier the age at which cannabis is first consumed, the greater the risk.
So, what might cannabis do that would cause psychosis in vulnerable individuals? THC will stimulate the cannabinoid receptors type 1 (CB1-R) , which are abundant in the cerebral cortex, particularly the frontal regions. basal ganglia, hippocampus, anterior cingular cortex and cerebellum. All of these areas can play a role in the neural circuitry of psychosis, and animal studies have implicated cannabis as a causative agent in the psychosis hotspot of the mesolimbic area.
Only a small proportion of cannabis users develop psychosis, suggesting there are genetic forces at play. The primary effect of endocannabinoid activation is the modulation of neurotransmitter release in the mesolimbic area. Animal studies also suggest that exogenous cannabinoids like THC affect dopaminergic transmission in the prefrontal cortex and the mesolimbic pathway (the areas affected by schizophrenia).
Let's examine COMT. This enzyme sits in the synapse and will break down dopamine, norepinephrine, and epinephrine. There is a common polymorphism of the COMT gene - folks with the valine allele of the COMT gene will have higher COMT function than those with the methionine allele. Increased COMT activity may result in a combination of reduced dopamine transmission in the prefrontal cortex and increased dopamine mesolimbic signaling - this combination is higher risk in schizophrenia, which presents with decreased executive functioning and working memory combined with risk of experiencing delusions and hallucinations.
Adolescents carrying the Val allele of the COMT gene are more at risk for schizophrenia in the Caspi research - the Sanjuan research found that those with the Met allele were more at risk. Other studies of cannabis use suggest that those with psychosis are more likely to use cannabis, and more likely to use the high-potency cannabis called "skunk."
That's all well and good. Repeated used of a cannabinoid agonist (POT) will produce prolonged and repeated use of the cannabinoid receptor. This will result in hunger, a bit of paranoia, psychosis, euphoria, cognitive impairment, and pain relief, and withdrawal effects of increased pain and anxiety.
So, does cannabis use increase the risk of schizophrenia use or what? Well, all the studies are observational, and it is pretty clear that those at risk for psychosis (with prodromal symptoms and high genetic risk) will tend to use more cannabis. However, the strongest evidence against a causative effect of cannabis is from native populations who regularly use cannabis, and in which there is no increased risk of psychosis. Your risk will depend upon your genes and experience- but I am not a fan.
That doesn't mean I don't push for elimination of food toxins, put in a little plug for pasture butter, demonstrate and encourage stress reduction techniques, focus on good sleep hygiene (and look for sleep disturbance and medical causes), and I do take people off statins when there is good clinical reason (primarily in folks with dementia, with good results, actually. Also, a couple of cases of resistant depression.) But I can't go full-blown evolutionary psychiatry with all my patients. Some aren't interested, and for others the data isn't there. Which is okay. EvPsych has reinvigorated my interest in the field and in research, and I feel the preventative potential of a paleo 2.0 diet is amazing - so for subclinical disease, I feel my blog and the diet are likely doing a lot of good, far more good than I could do in the time I have to see patients one by one. But I don't have any proof of that. Which is okay. I'll still keep looking for more evidence and more nutritional links.
But! Cannabis! I am honored that my twitter feed (warning - I might tweet about Crossfit, shampoo, and my children) is followed by Dr. Sanjuan in Spain, who sent me a link to this article, which among other articles will be the anchor for this post.
Cannabis. Evo Med is the province of rebels, and rebels love pot...
Pot might not love you.
Cannabis is the world's most popular recreational drug and its use has accelerated among adolescents in the United States.
There are two circumstances in which I tend to see heavy pot use - young people struggling with psychotic disorders, and older folks with lifetime heavy pot use struggling with cognitive function and anxiety problems. Such circumstances are weighted to bias my opinion against pot as the happy self-medication of choice. You are forewarned!
Cannabis use has a high comorbidity with populations with psychotic disorders. Its continued use is associated with poor outcomes in psychosis and with more frequent and earlier relapses (1). Use has been associated as a risk factor for emerging psychosis, and a young person with heavy use will have a two-fold risk of developing psychosis (2)(3). The earlier the age at which cannabis is first consumed, the greater the risk.
So, what might cannabis do that would cause psychosis in vulnerable individuals? THC will stimulate the cannabinoid receptors type 1 (CB1-R) , which are abundant in the cerebral cortex, particularly the frontal regions. basal ganglia, hippocampus, anterior cingular cortex and cerebellum. All of these areas can play a role in the neural circuitry of psychosis, and animal studies have implicated cannabis as a causative agent in the psychosis hotspot of the mesolimbic area.
Only a small proportion of cannabis users develop psychosis, suggesting there are genetic forces at play. The primary effect of endocannabinoid activation is the modulation of neurotransmitter release in the mesolimbic area. Animal studies also suggest that exogenous cannabinoids like THC affect dopaminergic transmission in the prefrontal cortex and the mesolimbic pathway (the areas affected by schizophrenia).
Let's examine COMT. This enzyme sits in the synapse and will break down dopamine, norepinephrine, and epinephrine. There is a common polymorphism of the COMT gene - folks with the valine allele of the COMT gene will have higher COMT function than those with the methionine allele. Increased COMT activity may result in a combination of reduced dopamine transmission in the prefrontal cortex and increased dopamine mesolimbic signaling - this combination is higher risk in schizophrenia, which presents with decreased executive functioning and working memory combined with risk of experiencing delusions and hallucinations.
Adolescents carrying the Val allele of the COMT gene are more at risk for schizophrenia in the Caspi research - the Sanjuan research found that those with the Met allele were more at risk. Other studies of cannabis use suggest that those with psychosis are more likely to use cannabis, and more likely to use the high-potency cannabis called "skunk."
That's all well and good. Repeated used of a cannabinoid agonist (POT) will produce prolonged and repeated use of the cannabinoid receptor. This will result in hunger, a bit of paranoia, psychosis, euphoria, cognitive impairment, and pain relief, and withdrawal effects of increased pain and anxiety.
So, does cannabis use increase the risk of schizophrenia use or what? Well, all the studies are observational, and it is pretty clear that those at risk for psychosis (with prodromal symptoms and high genetic risk) will tend to use more cannabis. However, the strongest evidence against a causative effect of cannabis is from native populations who regularly use cannabis, and in which there is no increased risk of psychosis. Your risk will depend upon your genes and experience- but I am not a fan.
Saturday, May 14, 2011
Inositol - The Nervous System's Pony Express
At long last! Between Blogger going kaput for a couple of days and the usual stuff, my inositol post had to wait a bit. I'm sure more people are interested in cannabis, but those are a few days away, assuming I don't get distracted by something else along the way (as is so often the case).
Anyway, the research team at Massachusetts General Hospital (I attended some of their meetings when I was a resident) just published a good paper in the Journal of Affective Disorders: Second-tier natural antidepressants: Review and critique. This paper goes over R. rosea, chromium, 5-HTP, and inositol, but I'm going to start with inositol, as I could use some second messaging review myself, and I looked it up specifically for a patient as well. Even though we are talking "natural" supplements here I still don't contend this is "evolutionary" psychiatry - none of our ancestors were chugging vats of inositol so far as I know - but figuring out how these things work helps us to understand biochemistry and speculate as to what could be going on that we might end up with an inositol deficiency, as it were.
First off - let's just mention the "first tier" natural antidepressants and complementary medicine treatments. That is, stuff generally considered "herbals" or "alternative medicine" that has a solid evidence base in the scientific literature. (I'm using the "quotes" because I don't see the need to distinguish these things so much - is there evidence base or not? I don't care if someone thinks meditation is flakey or "new age" - does it work? It certainly can! With life-changing results. Off my high horse). The well-studied "herbals" with a "growing consensus of antidepressant effectiveness and safety" include St. John's Wort*, SAMe, and omega-3 fatty acids. Folate, acupuncture, and exercise are other alternative treatments that have some studies of efficacy as antidepressants.
So, inositol doesn't have as much evidence base as any of the treatments in the previous paragraph, but we'll talk about what it is, and the evidence we have. (SAMe has shown efficacy in at least 20 trials over the years, some larger than others, some better controlled than others, so it is my "favorite" alternative treatment - but it can cause mania, and unless your folate cycle is humming along, can become evil homocysteine, so be warned).
So - inositol is a sugar alcohol and an isomer of glucose, and its 9 varieties are found mostly within cell membranes. Myo-inositol is the most abundant stereoisomer, making up 95% of the total free inositol in the body. Humans generally consume about a gram of inositol a day, and it is abundant in grains, beans, nuts, and fruits. (You might not be surprised to know the best sources are organ meats - beef heart and liver, but also wheat germ - but, uh oh - wouldn't the phytic acid in wheat germ bind up inositol - well, inositol is a part of phytic acid, which we can't actually break down, so, typically, animal sources will be more bioavailable than the phytate plant sources of inositol.) However, I ain't gonna lie - we can make inositol from glucose, and there's no evidence that we have a limited capacity to make inositol so that a dietary deficiency may not matter. We eat maybe a gram a day, and our kidneys make about 2 grams a day. Inositol is sometimes called "Vitamin B8."
So what does inositol do in the human body? Well, tons of things, actually. It is a key part of the second messenger system. Que? Well, in the pony express line that is a cell, surface proteins and receptor complexes (the mailer) hand off signals to the second messengers (the riders on the ponies) who pass the signal along eventually to other cell systems (the message recipients), such as the nucleus. All the major neurotransmitter systems use inositol as part of their messaging line - I'm talking dopamine, norepinephrine, serotonin, acetylcholine… "The potential importance of inositol in psychiatric disorders is thereby evident when one considers the number of receptor types/subtypes that interact with this signal transduction pathway."
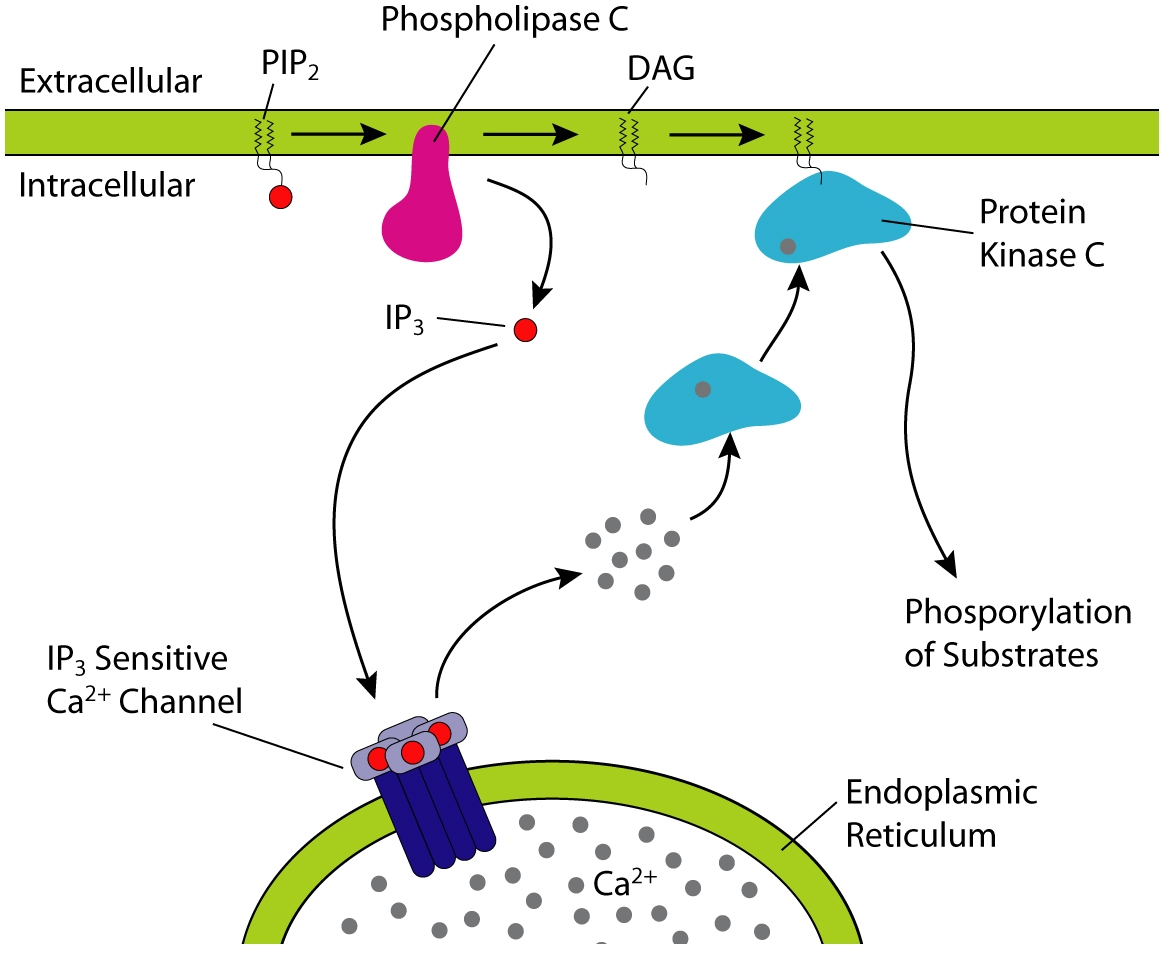
Biochem nerds will already know this next bit, but biochem nerd wanna-be's listen up (the rest of you can skip to after the picture, because this bit is a little dry) => Inositol is used to make inositol triphosphate (IP3) and diacylglycerol (DAG). IP3 binds IP3 receptors, particularly calcium channels in the endoplasmic reticulum, which will cause calcium levels in the cytoplasm to increase, causing a cascade of intracellular activity. Calcium and DAG can activate protein kinase C, which (as all kinases do) goes around sticking phosphates on things, leading to altered activity. Anyone learning molecular biology and biochemistry will see this pathway mentioned so many times your eyeballs will glaze over. So, in short, inositol is vital.
Picture! (from wikipedia):

There has been discussion in the comments on my lithium posts about lithium interfering with inositol metabolism - specifically it interferes with inositol monophosphatase possibly leading to reduced recycling of inositol and IP3 in the cell and reduced inositol levels (1) however - it is unclear that the actual end product is a reduction of second messenging or something else. One theory of bipolar disorder is that it is caused by "hyperkinetic second messenger systems." This imaging study seems to confirm that something screwy is going on with second messenger systems in bipolar disorder, but no one is sure yet what the heck it all means. By this same theory, the "depression" side of bipolar disorder might result from a reduction of inositol after the manic episodes, and depressive disorders might result from reduced signaling in the first place, leading to inefficient cell energetics, mechanics, and build-up of toxic calcium in the wrong places at the wrong times. Sounds nasty.
Ready for the clinical data (ie the really interesting and more practical stuff)?? A study back in 1978 found decreased inositol levels in the spinal fluid of depressed patients. However, subsequent studies didn't replicate the finding, and that levels of inositol in the spinal fluid didn't predict response to inositol. But post-mortem examination of suicide victims have shown lowered myo-inositol levels, and magnetic resonance spectroscopy showed reduced myo-inositol levels in the frontal lobes of bipolar and unipolar depressed patients. Dietary administration has been shown to increase inositol concentration within the central nervous system in humans (2).
But does it work? In the comments, more than once people have mentioned taking inositol 750mg several times a day with good effect. Well, there are a number of trials, some controlled, some open-label. In the trials, an average dose was 12 GRAMS a day (which would be 16 of those 750mg capsules - divided 2-4 times a day - which would mean you would go through this bottle in a little over six days, putting the monthly cost minus shipping at about $34… inositol is also available as a powder which seems like it could be a bit more cost-effective for the "prescription" doses studied). Some trials showed no benefit, but others showed no improvement at 2 weeks, but a definite improvement at 4 weeks. Trials (as an adjunctive treatment, meaning with mood stabilizers) in bipolar depression were a little more promising. One patient did develop mania after 24 weeks on inositol. Most of these studies were done on people who did not respond to traditional antidepressants, and so even a modest effect is promising, as so-called "treatment resistant" patients tend to be "treatment resistant" to all kinds of interventions. Additional studies (typically using even more inositol - 18 grams a day) had positive results for anxiety, bulimia, and obsessive compulsive disorder. Inositol seems to act on these disorders a bit like nature's SSRI.
What is inositol's downside (besides needing to take mountains of it) - side effects in these trials included mild increases in plasma glucose, gas, nausea, sleepiness, insomnia, dizziness, and headache, and then there are the case reports of mania (any antidepressant, including light therapy, can cause mania in vulnerable people.) No one dropped out of the trials due to side effects from inositol. Inositol does not appear to have any drug-drug interactions - however, it might induce uterine contractions in pregnant women, so should not be used in pregnancy (3).
In the end, inositol might be helpful for some people, and it would be interesting to see if the organ-meat eating paleos have higher inositol levels in the CNS than your average grain eater. But you'd have to eat a lot of beef heart to reach 12 grams daily.
*about St. John's Wort - product studies I have seen in the past suggest you are unlikely to get standard doses or product in SJW off the shelf, also it is most probably an MAOI and definitely has major drug interactions, such as with birth control pills and coumadin - SJW is not a product I routinely recommend for those reasons - BUT in the RCTs of pharmaceutical grade - one of which was done by this same Massachusetts General Hospital research group- it worked as well as prescription antidepressants. Chris Kresser suggests that this is because they all work as well as placebo. Personally I think from reviews of published and unpublished studies prescription antidepressants give you a 10% advantage over placebo in the short term and likely work better in the long term, but they are a pain in many ways, have side effects, and the long-term effects are generally unknown… my favorite source for unbiased evidenced-based information on psychiatric meds is Dr. Daniel Carlat his team at The Carlat Report. He has a great blog focused on industry influence and sniffing out misleading information but it is geared more toward psychiatrists than the layperson.
Anyway, the research team at Massachusetts General Hospital (I attended some of their meetings when I was a resident) just published a good paper in the Journal of Affective Disorders: Second-tier natural antidepressants: Review and critique. This paper goes over R. rosea, chromium, 5-HTP, and inositol, but I'm going to start with inositol, as I could use some second messaging review myself, and I looked it up specifically for a patient as well. Even though we are talking "natural" supplements here I still don't contend this is "evolutionary" psychiatry - none of our ancestors were chugging vats of inositol so far as I know - but figuring out how these things work helps us to understand biochemistry and speculate as to what could be going on that we might end up with an inositol deficiency, as it were.
First off - let's just mention the "first tier" natural antidepressants and complementary medicine treatments. That is, stuff generally considered "herbals" or "alternative medicine" that has a solid evidence base in the scientific literature. (I'm using the "quotes" because I don't see the need to distinguish these things so much - is there evidence base or not? I don't care if someone thinks meditation is flakey or "new age" - does it work? It certainly can! With life-changing results. Off my high horse). The well-studied "herbals" with a "growing consensus of antidepressant effectiveness and safety" include St. John's Wort*, SAMe, and omega-3 fatty acids. Folate, acupuncture, and exercise are other alternative treatments that have some studies of efficacy as antidepressants.
So, inositol doesn't have as much evidence base as any of the treatments in the previous paragraph, but we'll talk about what it is, and the evidence we have. (SAMe has shown efficacy in at least 20 trials over the years, some larger than others, some better controlled than others, so it is my "favorite" alternative treatment - but it can cause mania, and unless your folate cycle is humming along, can become evil homocysteine, so be warned).
So - inositol is a sugar alcohol and an isomer of glucose, and its 9 varieties are found mostly within cell membranes. Myo-inositol is the most abundant stereoisomer, making up 95% of the total free inositol in the body. Humans generally consume about a gram of inositol a day, and it is abundant in grains, beans, nuts, and fruits. (You might not be surprised to know the best sources are organ meats - beef heart and liver, but also wheat germ - but, uh oh - wouldn't the phytic acid in wheat germ bind up inositol - well, inositol is a part of phytic acid, which we can't actually break down, so, typically, animal sources will be more bioavailable than the phytate plant sources of inositol.) However, I ain't gonna lie - we can make inositol from glucose, and there's no evidence that we have a limited capacity to make inositol so that a dietary deficiency may not matter. We eat maybe a gram a day, and our kidneys make about 2 grams a day. Inositol is sometimes called "Vitamin B8."
So what does inositol do in the human body? Well, tons of things, actually. It is a key part of the second messenger system. Que? Well, in the pony express line that is a cell, surface proteins and receptor complexes (the mailer) hand off signals to the second messengers (the riders on the ponies) who pass the signal along eventually to other cell systems (the message recipients), such as the nucleus. All the major neurotransmitter systems use inositol as part of their messaging line - I'm talking dopamine, norepinephrine, serotonin, acetylcholine… "The potential importance of inositol in psychiatric disorders is thereby evident when one considers the number of receptor types/subtypes that interact with this signal transduction pathway."
Biochem nerds will already know this next bit, but biochem nerd wanna-be's listen up (the rest of you can skip to after the picture, because this bit is a little dry) => Inositol is used to make inositol triphosphate (IP3) and diacylglycerol (DAG). IP3 binds IP3 receptors, particularly calcium channels in the endoplasmic reticulum, which will cause calcium levels in the cytoplasm to increase, causing a cascade of intracellular activity. Calcium and DAG can activate protein kinase C, which (as all kinases do) goes around sticking phosphates on things, leading to altered activity. Anyone learning molecular biology and biochemistry will see this pathway mentioned so many times your eyeballs will glaze over. So, in short, inositol is vital.
Picture! (from wikipedia):
{kind=link}

There has been discussion in the comments on my lithium posts about lithium interfering with inositol metabolism - specifically it interferes with inositol monophosphatase possibly leading to reduced recycling of inositol and IP3 in the cell and reduced inositol levels (1) however - it is unclear that the actual end product is a reduction of second messenging or something else. One theory of bipolar disorder is that it is caused by "hyperkinetic second messenger systems." This imaging study seems to confirm that something screwy is going on with second messenger systems in bipolar disorder, but no one is sure yet what the heck it all means. By this same theory, the "depression" side of bipolar disorder might result from a reduction of inositol after the manic episodes, and depressive disorders might result from reduced signaling in the first place, leading to inefficient cell energetics, mechanics, and build-up of toxic calcium in the wrong places at the wrong times. Sounds nasty.
Ready for the clinical data (ie the really interesting and more practical stuff)?? A study back in 1978 found decreased inositol levels in the spinal fluid of depressed patients. However, subsequent studies didn't replicate the finding, and that levels of inositol in the spinal fluid didn't predict response to inositol. But post-mortem examination of suicide victims have shown lowered myo-inositol levels, and magnetic resonance spectroscopy showed reduced myo-inositol levels in the frontal lobes of bipolar and unipolar depressed patients. Dietary administration has been shown to increase inositol concentration within the central nervous system in humans (2).
But does it work? In the comments, more than once people have mentioned taking inositol 750mg several times a day with good effect. Well, there are a number of trials, some controlled, some open-label. In the trials, an average dose was 12 GRAMS a day (which would be 16 of those 750mg capsules - divided 2-4 times a day - which would mean you would go through this bottle in a little over six days, putting the monthly cost minus shipping at about $34… inositol is also available as a powder which seems like it could be a bit more cost-effective for the "prescription" doses studied). Some trials showed no benefit, but others showed no improvement at 2 weeks, but a definite improvement at 4 weeks. Trials (as an adjunctive treatment, meaning with mood stabilizers) in bipolar depression were a little more promising. One patient did develop mania after 24 weeks on inositol. Most of these studies were done on people who did not respond to traditional antidepressants, and so even a modest effect is promising, as so-called "treatment resistant" patients tend to be "treatment resistant" to all kinds of interventions. Additional studies (typically using even more inositol - 18 grams a day) had positive results for anxiety, bulimia, and obsessive compulsive disorder. Inositol seems to act on these disorders a bit like nature's SSRI.
What is inositol's downside (besides needing to take mountains of it) - side effects in these trials included mild increases in plasma glucose, gas, nausea, sleepiness, insomnia, dizziness, and headache, and then there are the case reports of mania (any antidepressant, including light therapy, can cause mania in vulnerable people.) No one dropped out of the trials due to side effects from inositol. Inositol does not appear to have any drug-drug interactions - however, it might induce uterine contractions in pregnant women, so should not be used in pregnancy (3).
In the end, inositol might be helpful for some people, and it would be interesting to see if the organ-meat eating paleos have higher inositol levels in the CNS than your average grain eater. But you'd have to eat a lot of beef heart to reach 12 grams daily.
*about St. John's Wort - product studies I have seen in the past suggest you are unlikely to get standard doses or product in SJW off the shelf, also it is most probably an MAOI and definitely has major drug interactions, such as with birth control pills and coumadin - SJW is not a product I routinely recommend for those reasons - BUT in the RCTs of pharmaceutical grade - one of which was done by this same Massachusetts General Hospital research group- it worked as well as prescription antidepressants. Chris Kresser suggests that this is because they all work as well as placebo. Personally I think from reviews of published and unpublished studies prescription antidepressants give you a 10% advantage over placebo in the short term and likely work better in the long term, but they are a pain in many ways, have side effects, and the long-term effects are generally unknown… my favorite source for unbiased evidenced-based information on psychiatric meds is Dr. Daniel Carlat his team at The Carlat Report. He has a great blog focused on industry influence and sniffing out misleading information but it is geared more toward psychiatrists than the layperson.
Wednesday, May 11, 2011
Couple Things...
I have some more refurbished posts up on Psychology Today - some are updated, and/or combined posts, and a couple of them have some pretty intense information that deserves a refresher even if you have read it before ;-)
Autism and Ketogenic Diets
ADHD and Mom's Serotonin Deficiency
Sunlight, Sugar, and Serotonin
Also, a big thanks to the lovely people at the British Journal of Psychiatry, who have granted me persmission to use their graph in my Season of Birth and Anorexia Nervosa post from the end of last month.
As for new stuff, I'll likely have a post on inositol (and its uses for depression) up in the next day or two, followed by some cannabis posts.
Happy Wednesday!
Autism and Ketogenic Diets
ADHD and Mom's Serotonin Deficiency
Sunlight, Sugar, and Serotonin
Also, a big thanks to the lovely people at the British Journal of Psychiatry, who have granted me persmission to use their graph in my Season of Birth and Anorexia Nervosa post from the end of last month.
As for new stuff, I'll likely have a post on inositol (and its uses for depression) up in the next day or two, followed by some cannabis posts.
Happy Wednesday!
Saturday, May 7, 2011
What We Do Can Change the Brain - Trauma, Genes, and Epigenetics
Back in 2003, Avshalom Caspi published a paper in Science that rocked everyone's world (at least in psychiatry): Influence of Life Stress on Depression: Moderation by a Polymorphism in the 5-HTT Gene.
Y'all remember Lamarck, right? He's the guy who postulated that giraffe's necks got all long because they stretched them to reach the high leaves, and the stretchiness-length was passed on to baby giraffes. Well, it turns out that in some respect, Lamarck had it right - what we do, what we eat, what we experience, how we cope - all of these things can affect the expression of our DNA. So Lamarck gets the last laugh - to some extent. You want to change those brown eyes blue - don't wait for Lamarck - get some contacts. And don't expect the kids to inherit the faux color.
And so at last we come around to Evolutionary Psychiatry. Our gene expression has been modulated by selection pressure for thousands and thousands of human generations. Live and eat and sleep more like a hunter-gatherer, and it seems to me you are more likely to deactivate the histones for the genes for survival, strength, resilience, and happiness. When you are the most resilient you can be, presumably you raise little resilient humans to take your place.
And some things we cannot change. If I'm a l/l, theoretically I can deal with more stress than an s/s without being depressed - but of course, many of the s/s cohort had no depressive episodes, despite having 4 or more stressful life events. But why has s/s been maintained in the population despite serving up a higher risk of suicide and depression in combination with stress? Well, the most likely explanation is that the short allele of the serotonin reuptake transporter promoter gives us some sort of resistance to disease (1). But who knows. In the mean time, I'll try to limit my stress and eat more like a hunter-gatherer.
I know that doesn't sound all that exciting, but everyone who is anyone will pull a graph from this 4-page seminal Caspi work and ooh and aww over it. In fact, as of this week, the article has been cited by 2022 other articles. This paper links nature and nurture and depression in one elegant demonstration - so without further ado…
Caspi used subjects from a lifelong observational study, the white New Zealanders known as the Dunedin Multidisciplinary Health and Development Study. This cohort of 1037 children was studied at ages 3,5,7,9,11,13,15, 18, and 21, and 96% of the subjects could still be found at the age of 26. This careful observation meant that Caspi could not only rely on the lifelong memories of the subjects about history of trauma and medical/depressive issues (which can be to some extent unreliable), but also what was studied at all the data points in the subject's lives.
847 members of the cohort were divided into three groups based on 5-HTTLPR genotype - l/l, s/s, and s/l. No need to scratch your head - let me explain!
Basically, we are talking serotonin here. Serotonin is an important neurotransmitter in regulating our emotional state. Like any neurotransmitter, serotonin is made by one neuron, which then spits it out into the synapse in between neurons. Then the serotonin floats over to the second neuron and activates the receptors over there. On the first neuron, there is a serotonin reuptake transporter that sucks serotonin back into the first neuron to be recycled and used again. See the picture below:
 |
| Image Credit |
{kind=link}
So peer at that reuptake transporter (yellow) and have a look. All of us have genes that code for the making of that transporter. And this gene happens to have a special promoter (called the 5HTTLPR) that directs how much serotonin reuptake transporter we make. People (and rhesus monkeys, as it happens) that have two LONG (l/l) copies of the promoter have higher levels of serotonin in the spinal fluid. People (and monkeys) with two SHORT (s/s) copies of the promoter have lower levels of serotonin in the spinal fluid. People with a short and a long (s/l) are, predictably, intermediate. Got it? Serotonin-speaking, s/s is the short end of the stick, s/l is in the middle, and l/l is protective.
Back to New Zealand, where it was found that 17% of the young adults in the Dunedin cohort were s/s, 51% were s/l, and 31% were l/l. Caspi and his crew collected information about previous depressive episodes, suicide attempts, previous traumatic events (employment, financial, housing, health, and relationship stressors), and current psychological state. It turns out that when you look at current or previous depression or suicide attempts, the link between the type of promoter you have and those findings are non-significant. Uh oh. That sounds like a big bust! The type of serotonin transporter gene promoter you have doesn't seem to matter…
Then Caspi's team ran the numbers backwards and forwards, plugged in number of stressful life events and generated this remarkable finding:

As you can see, if you've had no stressful life events, your likelihood of having a depressive episode is around 10%. If you have the protective l/l version of the promoter, even if you have 4+ major stressful events, your chance of having a depressive episode only climbs a little. But if you have the s/s "short end of the stick" promoter, add stress and your risk of developing depression climbs very quickly. When you plug in severe childhood maltreatment as a variable, the s/s folks have a 63% chance of having a major depressive episode by age 26. The l/l severely maltreated children had a 30% risk of having a major depressive episode by age 26. The s/s folks with 4 or more stressful life events accounted for only 10% of the cohort, but 23% of the cases of diagnosed depression in the cohort.
So what we have found here is that this particular genetic lottery can tell us to some extent which of us are more resilient to stress, and which of us are less so, at least with respect to depressive episodes and suicide attempts (plotting suicide attempts against number of stressful life events generates a similar graph). These percentages (roughly 20% s/s, 50% s/l, and 30% l/l) are pretty much the same as those in Europe and America. The yearly incidence of Major Depressive Disorder is right around 20% too, by the way.
Back to New Zealand, where it was found that 17% of the young adults in the Dunedin cohort were s/s, 51% were s/l, and 31% were l/l. Caspi and his crew collected information about previous depressive episodes, suicide attempts, previous traumatic events (employment, financial, housing, health, and relationship stressors), and current psychological state. It turns out that when you look at current or previous depression or suicide attempts, the link between the type of promoter you have and those findings are non-significant. Uh oh. That sounds like a big bust! The type of serotonin transporter gene promoter you have doesn't seem to matter…
Then Caspi's team ran the numbers backwards and forwards, plugged in number of stressful life events and generated this remarkable finding:

As you can see, if you've had no stressful life events, your likelihood of having a depressive episode is around 10%. If you have the protective l/l version of the promoter, even if you have 4+ major stressful events, your chance of having a depressive episode only climbs a little. But if you have the s/s "short end of the stick" promoter, add stress and your risk of developing depression climbs very quickly. When you plug in severe childhood maltreatment as a variable, the s/s folks have a 63% chance of having a major depressive episode by age 26. The l/l severely maltreated children had a 30% risk of having a major depressive episode by age 26. The s/s folks with 4 or more stressful life events accounted for only 10% of the cohort, but 23% of the cases of diagnosed depression in the cohort.
So what we have found here is that this particular genetic lottery can tell us to some extent which of us are more resilient to stress, and which of us are less so, at least with respect to depressive episodes and suicide attempts (plotting suicide attempts against number of stressful life events generates a similar graph). These percentages (roughly 20% s/s, 50% s/l, and 30% l/l) are pretty much the same as those in Europe and America. The yearly incidence of Major Depressive Disorder is right around 20% too, by the way.
We've learned also that trauma changes our brain. Years later, if we have endured trauma, we are more vulnerable to having a major depressive episode and to make suicide attempts, modulated in part by how many serotonin reuptake transporters we have.
How does trauma change the brain? Our genes are pretty much set in stone from the moment 23 chromosomes from Mama meet 23 from Dada (except for random mutations). However, gene expression can change throughout life (and over generations). How does that happen? Well, that's (in part) what we mean by the word epigenetics.
A lot of our DNA spends its life wrapped up like candy. Proteins called histones wrap around the DNA and prevent it from being transcribed into RNA (RNA is the stuff that is eventually translated into proteins). Histone wrapping is entirely necessary - after all, all of our cells (except sperm and eggs) have the same DNA, and yet it is patently obvious that a skin cell is quite different from an eyeball cell which is different than a neuron. So in some cells, certain DNA is expressed, but not in other cells.
Histones that are highly methylated hang on tight to the DNA and keep it from being transcribed. Once you demethylate the histones, the DNA is set free to be expressed. A practical example - certain species of rodents called voles have species that have very attentive mothers, and less attentive mothers. The baby voles raised by the less attentive mothers seem to be more vulnerable to stress later in life. But put a less attentive species vole with a high attentive species mother, and the baby vole grows up resilient to stress. Decreased methylation of the attentive (oxytocin) gene results in a genetically inattentive vole becoming more like an attentive vole.
How does trauma change the brain? Our genes are pretty much set in stone from the moment 23 chromosomes from Mama meet 23 from Dada (except for random mutations). However, gene expression can change throughout life (and over generations). How does that happen? Well, that's (in part) what we mean by the word epigenetics.
A lot of our DNA spends its life wrapped up like candy. Proteins called histones wrap around the DNA and prevent it from being transcribed into RNA (RNA is the stuff that is eventually translated into proteins). Histone wrapping is entirely necessary - after all, all of our cells (except sperm and eggs) have the same DNA, and yet it is patently obvious that a skin cell is quite different from an eyeball cell which is different than a neuron. So in some cells, certain DNA is expressed, but not in other cells.
Histones that are highly methylated hang on tight to the DNA and keep it from being transcribed. Once you demethylate the histones, the DNA is set free to be expressed. A practical example - certain species of rodents called voles have species that have very attentive mothers, and less attentive mothers. The baby voles raised by the less attentive mothers seem to be more vulnerable to stress later in life. But put a less attentive species vole with a high attentive species mother, and the baby vole grows up resilient to stress. Decreased methylation of the attentive (oxytocin) gene results in a genetically inattentive vole becoming more like an attentive vole.
Y'all remember Lamarck, right? He's the guy who postulated that giraffe's necks got all long because they stretched them to reach the high leaves, and the stretchiness-length was passed on to baby giraffes. Well, it turns out that in some respect, Lamarck had it right - what we do, what we eat, what we experience, how we cope - all of these things can affect the expression of our DNA. So Lamarck gets the last laugh - to some extent. You want to change those brown eyes blue - don't wait for Lamarck - get some contacts. And don't expect the kids to inherit the faux color.
And so at last we come around to Evolutionary Psychiatry. Our gene expression has been modulated by selection pressure for thousands and thousands of human generations. Live and eat and sleep more like a hunter-gatherer, and it seems to me you are more likely to deactivate the histones for the genes for survival, strength, resilience, and happiness. When you are the most resilient you can be, presumably you raise little resilient humans to take your place.
And some things we cannot change. If I'm a l/l, theoretically I can deal with more stress than an s/s without being depressed - but of course, many of the s/s cohort had no depressive episodes, despite having 4 or more stressful life events. But why has s/s been maintained in the population despite serving up a higher risk of suicide and depression in combination with stress? Well, the most likely explanation is that the short allele of the serotonin reuptake transporter promoter gives us some sort of resistance to disease (1). But who knows. In the mean time, I'll try to limit my stress and eat more like a hunter-gatherer.
Thursday, May 5, 2011
Nature and Nurture - The Basis of Mental Illness
"So what's more important, doc? Genes or how you were raised?"
I'm asked that question or a variation thereof quite frequently. Some people wonder how much they can do to truly change, and others are concerned about the risk of mental illness their children might have. It's an important question, and while the simple answer is, "both are important," the complicated answer describes the very essence of the biology of psychopathology. And in that biology you also see the clues for cures.
So, yes, a molecular biology-heavy post. That calls for some music. Hmmm. The Airborne Toxic Event - Changing (right click to open in new tab).
Mental illness, as it turns out, has some of the highest genetic loading of any common illness*. Of course there are some rather famous single-gene disorders (like Huntington's or cystic fibrosis) whose risk seems to be almost entirely genetic, but right up there is schizophrenia, where 80% of the risk is genetic. That means if you have no relatives with schizophrenia, it is unlikely you will develop it. Genetic loading counts for a large portion of the risk for bipolar disorder and major depressive disorder as well.
Schizophrenia is the most studied of many of these disorders at a basic science level, I would say. And it is pretty clear that patients with schizophrenia and their close relatives have decreased prefrontal cortical efficiency. Since the prefrontal cortex is responsible for planning, elements of memory, controlling impulsivity, predicting outcomes, and many other important parts of thinking, having an inefficient cortex is very problematic, to say the least. Here's a slide showing the prefrontal network in schizophrenia:

You can click for a bigger version, of course, but the details aren't important for this blog post - the slide is really just a demonstration of the complexity and some of the neurons involved.
So, if schizophrenia is genetic, and we know the location in the brain where the first problems arise, can't we nail down the gene? In the last 5 years we've developed the capability to sequence genomes and check out genetic polymorphisms (differences in genes between one person and another) both rapidly and cheaply. This has enabled us to do a brute force hack of the genome, looking at the genes of many families and finding those genes that are common to families with schizophrenia and are absent in families without schizophrenia. I wrote about a similar study done for migraines a while back.
These types of genetic studies are fantastic - but you end up with tens of thousands of data points, so you can't possibly use the typical p value cut-off of 95% probability that the results are not due to chance (that's a decent enough definition for our purposes today - here's the real definition of p value). With that many data points and a p<0.05 cut-off, you are definitely going to end up with hundreds or even thousands of "statistically significant" correlations due to random chance. Therefore for studies like these, the cut-off is much, much smaller -- often <10 to the -8, for example.
Well, these studies have been done for schizophrenia, and two genes popped up, and they are not particularly exciting. Certain variants of the genes for NRGN and TGF4 were found to have an odds ratio of 1.21 and 1.33 for developing schizophrenia. That means if you have those genetic variants, instead of having a 0.5-1% of developing schizophrenia like the general population, you have a 0.6-1.2% chance of developing it (or thereabouts). So not a particularly risky genetic lot to draw!
What did we find out from these studies? Individual genes don't matter that much in the development of schizophrenia. But wait - didn't we just say that the risk for schizophrenia is 80% genetic? Well, let me throw out one more intimidating slide - a picture of the ErbB4 signaling pathway (this is just one bit of nerve signaling in certain areas, just one path by which signals get transmitted in a certain set of neurons - click for a better resolution, but again the big picture is far, far more important here than the details).

The Strokes - Under Cover of Darkness
The great thing about the brute force hack genetic studies is that if you have a computer, thousands of data points, and some grad students, you can just as easily look for correlations of not only 1, but 2 or 3 or 4 genetic polymorphisms. And when the schizophrenia researchers did that with the various genes associated with the ErbB4 signaling pathway, they hit the jackpot. All these genes interact with each other, like links in a chain. Break one link, and the brain can compensate. But break two links (so have two unfortunate genetic polymorphisms in this pathway), and your signaling becomes more inefficient. Your risk of schizophrenia goes up 8-fold. Break three links in the chain, and the risk for schizophrenia goes up 27-fold.
I'm using schizophrenia as an example - and many of the same genes and a severe inefficiency of the prefrontal cortical network are implicated in autism, by the way. Autism is likely to be, in a sense, a variant of schizophrenia that strikes much earlier in life. A similar story (but in different areas of the brain and with different specific signaling pathways) can be told for anxiety, depression, ADHD…
For heaven's sake I don't care how many rock songs you link, who cares and what does this have to do with nutrition and environment and blah blah blah…
All these pathways and all these signals have been running along using the nutrients and lifestyle we have evolved for thousands and thousands of generations. The signaling depends upon having magnesium, zinc, cholesterol, omega 3s and arachidonic acid, vitamin D, creatine, CoQ10, restorative sleep, appropriate lighting, proper energy efficiency and neuronal recovery and repair. Some of us are nearly bullet-proof. We have lickety-split efficient neural networks that seem to be able to run on garbage. Others of us have some sort of problem somewhere, and we need all our compensatory mechanisms working, and we need to give our neural networks all the raw materials in the right amounts.
My next post will focus more on depression, trauma, and the nitty-gritty of epigenetics. In the mean time let me reiterate:
What we do matters. What we eat matters. To be the optimal human being from the genetic hand we were given, we'd best live in a way that compliments our biochemical programming.
* Much of the information I'm presenting today is from lectures I attended last week by Carl Salzman, MD (of Harvard), Jeffrey Lieberman MD (of Columbia), and Daniel Weinberger MD (of NIMH and NIH) - all are world famous researchers in psychosis and psychiatry. I had the pleasure of attending many lectures by Dr. Salzman during my residency. These lectures were not sponsored in any fashion by the pharmaceutical industry.
I'm asked that question or a variation thereof quite frequently. Some people wonder how much they can do to truly change, and others are concerned about the risk of mental illness their children might have. It's an important question, and while the simple answer is, "both are important," the complicated answer describes the very essence of the biology of psychopathology. And in that biology you also see the clues for cures.
So, yes, a molecular biology-heavy post. That calls for some music. Hmmm. The Airborne Toxic Event - Changing (right click to open in new tab).
Mental illness, as it turns out, has some of the highest genetic loading of any common illness*. Of course there are some rather famous single-gene disorders (like Huntington's or cystic fibrosis) whose risk seems to be almost entirely genetic, but right up there is schizophrenia, where 80% of the risk is genetic. That means if you have no relatives with schizophrenia, it is unlikely you will develop it. Genetic loading counts for a large portion of the risk for bipolar disorder and major depressive disorder as well.
Schizophrenia is the most studied of many of these disorders at a basic science level, I would say. And it is pretty clear that patients with schizophrenia and their close relatives have decreased prefrontal cortical efficiency. Since the prefrontal cortex is responsible for planning, elements of memory, controlling impulsivity, predicting outcomes, and many other important parts of thinking, having an inefficient cortex is very problematic, to say the least. Here's a slide showing the prefrontal network in schizophrenia:

You can click for a bigger version, of course, but the details aren't important for this blog post - the slide is really just a demonstration of the complexity and some of the neurons involved.
So, if schizophrenia is genetic, and we know the location in the brain where the first problems arise, can't we nail down the gene? In the last 5 years we've developed the capability to sequence genomes and check out genetic polymorphisms (differences in genes between one person and another) both rapidly and cheaply. This has enabled us to do a brute force hack of the genome, looking at the genes of many families and finding those genes that are common to families with schizophrenia and are absent in families without schizophrenia. I wrote about a similar study done for migraines a while back.
These types of genetic studies are fantastic - but you end up with tens of thousands of data points, so you can't possibly use the typical p value cut-off of 95% probability that the results are not due to chance (that's a decent enough definition for our purposes today - here's the real definition of p value). With that many data points and a p<0.05 cut-off, you are definitely going to end up with hundreds or even thousands of "statistically significant" correlations due to random chance. Therefore for studies like these, the cut-off is much, much smaller -- often <10 to the -8, for example.
Well, these studies have been done for schizophrenia, and two genes popped up, and they are not particularly exciting. Certain variants of the genes for NRGN and TGF4 were found to have an odds ratio of 1.21 and 1.33 for developing schizophrenia. That means if you have those genetic variants, instead of having a 0.5-1% of developing schizophrenia like the general population, you have a 0.6-1.2% chance of developing it (or thereabouts). So not a particularly risky genetic lot to draw!
What did we find out from these studies? Individual genes don't matter that much in the development of schizophrenia. But wait - didn't we just say that the risk for schizophrenia is 80% genetic? Well, let me throw out one more intimidating slide - a picture of the ErbB4 signaling pathway (this is just one bit of nerve signaling in certain areas, just one path by which signals get transmitted in a certain set of neurons - click for a better resolution, but again the big picture is far, far more important here than the details).

The Strokes - Under Cover of Darkness
The great thing about the brute force hack genetic studies is that if you have a computer, thousands of data points, and some grad students, you can just as easily look for correlations of not only 1, but 2 or 3 or 4 genetic polymorphisms. And when the schizophrenia researchers did that with the various genes associated with the ErbB4 signaling pathway, they hit the jackpot. All these genes interact with each other, like links in a chain. Break one link, and the brain can compensate. But break two links (so have two unfortunate genetic polymorphisms in this pathway), and your signaling becomes more inefficient. Your risk of schizophrenia goes up 8-fold. Break three links in the chain, and the risk for schizophrenia goes up 27-fold.
I'm using schizophrenia as an example - and many of the same genes and a severe inefficiency of the prefrontal cortical network are implicated in autism, by the way. Autism is likely to be, in a sense, a variant of schizophrenia that strikes much earlier in life. A similar story (but in different areas of the brain and with different specific signaling pathways) can be told for anxiety, depression, ADHD…
For heaven's sake I don't care how many rock songs you link, who cares and what does this have to do with nutrition and environment and blah blah blah…
All these pathways and all these signals have been running along using the nutrients and lifestyle we have evolved for thousands and thousands of generations. The signaling depends upon having magnesium, zinc, cholesterol, omega 3s and arachidonic acid, vitamin D, creatine, CoQ10, restorative sleep, appropriate lighting, proper energy efficiency and neuronal recovery and repair. Some of us are nearly bullet-proof. We have lickety-split efficient neural networks that seem to be able to run on garbage. Others of us have some sort of problem somewhere, and we need all our compensatory mechanisms working, and we need to give our neural networks all the raw materials in the right amounts.
My next post will focus more on depression, trauma, and the nitty-gritty of epigenetics. In the mean time let me reiterate:
What we do matters. What we eat matters. To be the optimal human being from the genetic hand we were given, we'd best live in a way that compliments our biochemical programming.
* Much of the information I'm presenting today is from lectures I attended last week by Carl Salzman, MD (of Harvard), Jeffrey Lieberman MD (of Columbia), and Daniel Weinberger MD (of NIMH and NIH) - all are world famous researchers in psychosis and psychiatry. I had the pleasure of attending many lectures by Dr. Salzman during my residency. These lectures were not sponsored in any fashion by the pharmaceutical industry.
Sunday, May 1, 2011
Diet and Violence 2
Back in Diet and Violence, I presented evidence from two decently-sized randomized controlled trials of adding a multivitamin/multimineral/essential fatty acid supplement to normal prison fare. The trials were done about 8 years apart and in different countries, yet came out with a similar conclusion. Actual violent/discipline-requiring incidents committed by the prisoners who took the supplements was reduced by about 1/3 compared to pre-supplement days, and in one study the placebo-taking prisoners had an increase in violent events, whereas the other study showed just a small change on placebo.
My conclusion - practically speaking, I hope that prisoners in the US get a supplement (come to think of it, I have a friend who is a doctor in the prison system - but she was asking me what I thought about recommendations for vitamin D, so maybe the official guidelines aren't solid. Hmmm. Time to fire off a facebook message). I don't care if it is the best pharmaceutical grade supplement on the planet, a month of supplementation can't be more costly than a couple of days in prison. And total number of days in prison and parole and solitary and all those situations are in part determined by prisoner behavior, I imagine. I'm guessing that prisoners receive the most horrendous, cheap, grain-and-soy and margarine foods imaginable. We have to "get tough on crime" after all. Our tax dollars at work.
Of course I am being far too sensible - from the article about the pioneering diet and violence researcher Gesch in Science in 2009:
But let's step back from pragmatism for a moment. Here's the real issue with the science I pursue, at least in the eyes of the medical establishment (also from the Science article):
Gesch began working with young offenders in the 80s as a social worker. He would invite groups over for home-cooked meals, (the goal being that the atmosphere would help them open up and share their troubles) and Gesch noticed that after a while, the kids would be "transformed...
Finally he was able to obtain funding for his 2002 study, now replicated, and at the same time Gesch gathered data for a second paper on how food choices of prisoners affected actual daily intake of nutrients. He found (not surprisingly) that, when they got the chance, prisoners would buy food like peanuts, chips, candy and cookies from the prison store, which would add to their daily intake of omega-6 oils, trans fats, grains, and sugar. In addition, though the prison diets were designed by institutional dietitians, most had suboptimal amounts of vitamin D (even compared to the lowly 400 IU recommended for people with little sun) and selenium, and the vegetarian and Muslim menus often had some suboptimal B vitamins and total calories.
Just want to mention here Schoenthaler's randomized controlled trial from 2000, of 80 six-twelve year old schoolchildren who had previously been disciplined at school in "working class" Hispanic neighborhoods of Phoenix - Schoenthaler notes that previous randomized controlled trials of supplementation of the RDA for prisoners resulted in a 40% decrease in number of violent acts - his results were a 47% decrease in violent acts among the supplemented kids compared to the placebo controls. I'd call that more replication. And a call for some serious multivitamin/multimineral/EFA supplementation action on a large scale in institutions such as prisons, especially where relatives are often not allowed to bring in outside food.
Of course, nutrition is only a part of the larger problem of violence and crime. But in institutions, it seems like a relatively 30-40% controllable part, if only common sense would prevail.
My conclusion - practically speaking, I hope that prisoners in the US get a supplement (come to think of it, I have a friend who is a doctor in the prison system - but she was asking me what I thought about recommendations for vitamin D, so maybe the official guidelines aren't solid. Hmmm. Time to fire off a facebook message). I don't care if it is the best pharmaceutical grade supplement on the planet, a month of supplementation can't be more costly than a couple of days in prison. And total number of days in prison and parole and solitary and all those situations are in part determined by prisoner behavior, I imagine. I'm guessing that prisoners receive the most horrendous, cheap, grain-and-soy and margarine foods imaginable. We have to "get tough on crime" after all. Our tax dollars at work.
Of course I am being far too sensible - from the article about the pioneering diet and violence researcher Gesch in Science in 2009:
"Decades of studies by Schoenthaler and others have supported a connection between nutrition and violence, but for a variety of reasons—some scientific, others political—it hasn’t yet translated into policy."
But let's step back from pragmatism for a moment. Here's the real issue with the science I pursue, at least in the eyes of the medical establishment (also from the Science article):
“This field has seen a lot of exaggerated claims and not enough solid placebo-controlled research,” says Eugene Arnold, a psychiatrist and former director of the Nisonger Center at Ohio State University, Columbus. Studies have shown that “there clearly is a connection” between nutrients and behavioral disorders—for example, between nutrition and depression— but rigorous research has been the exception, he says. Most studies of the effects of nutrition on antisocial behavior are dismissed because of poor experimental design. And Arnold notes that misleading claims by the booming nutrient supplement industry have brought the taint of pseudoscience to those studying diet and behavior. “Even good scientists in this field have been treated as guilty by association,” he says.
Gesch began working with young offenders in the 80s as a social worker. He would invite groups over for home-cooked meals, (the goal being that the atmosphere would help them open up and share their troubles) and Gesch noticed that after a while, the kids would be "transformed...
...becoming healthier and often abandoning the antisocial behaviors that had gotten them into trouble. He began to believe that shedding their scattershot diets of junk food was central to the behavioral shift, perhaps even more so than the family-like socializing. "
Finally he was able to obtain funding for his 2002 study, now replicated, and at the same time Gesch gathered data for a second paper on how food choices of prisoners affected actual daily intake of nutrients. He found (not surprisingly) that, when they got the chance, prisoners would buy food like peanuts, chips, candy and cookies from the prison store, which would add to their daily intake of omega-6 oils, trans fats, grains, and sugar. In addition, though the prison diets were designed by institutional dietitians, most had suboptimal amounts of vitamin D (even compared to the lowly 400 IU recommended for people with little sun) and selenium, and the vegetarian and Muslim menus often had some suboptimal B vitamins and total calories.
Just want to mention here Schoenthaler's randomized controlled trial from 2000, of 80 six-twelve year old schoolchildren who had previously been disciplined at school in "working class" Hispanic neighborhoods of Phoenix - Schoenthaler notes that previous randomized controlled trials of supplementation of the RDA for prisoners resulted in a 40% decrease in number of violent acts - his results were a 47% decrease in violent acts among the supplemented kids compared to the placebo controls. I'd call that more replication. And a call for some serious multivitamin/multimineral/EFA supplementation action on a large scale in institutions such as prisons, especially where relatives are often not allowed to bring in outside food.
Of course, nutrition is only a part of the larger problem of violence and crime. But in institutions, it seems like a relatively 30-40% controllable part, if only common sense would prevail.
Housecleaning
A little post to keep me somewhat organized - though in many respects I don't like organization as it stomps my thinking patterns a bit. However, as life gets more complex, organization keeps the head above water. So here we are!
1) Contacting me - through the Psychology Today blog and through some comments on this blog I do receive requests for contact. Unfortunately, these requests quickly drop off the top of my email list as I usually think - okay, will get back to that when I have time - and then I don't end up having time! I can tell you I am much, much more likely to answer a specific, narrow question that can be dealt with quickly, or anecdotes about how some aspect of paleolithic/traditional-style diets either worked or didn't work for you (best left in a comment for everyone!). Contacts that sound like you want a full psychiatric consultation will likely not be answered. I would love to help, but can't do a proper job of that without taking a lot of time that I typically do not have. Also, I'm not likely to do that without getting paid, and it's illegal and bad practice to do it (except in certain very specific contexts) in states where I am not licensed. I can't practice medicine over the internet. Typically, the questions are something like: "Have you heard of such and such supplement and what do you think of it? Or "do you know any other psychiatrists who practice like you do in [enter your city here]." The answer is usually no to both questions, for better or worse.
In addition, there are often transference issues and other relationship issues that are very important in psychiatric treatment and questions, and often someone will seek my help because their relationship with their doctor or therapist has something broken - I can tell you right off that I am not the solution in those cases - the best thing to do is to talk to your own doctor or therapist explicitly about the broken part. If a mental health professional doesn't jump on that as a very important and interesting part of your treatment, time to maybe look around for someone else (in your area). Often the most exciting and helpful changes occur after someone tells me how I am not helping them.
2) Comments on Old Posts - There are many fabulous, detailed comments left on old posts, and some with very good questions. If the winds are blowing right, sometimes I have the time to answer them - often I don't. I do generally address questions in comments left in the most recent posts.
3) To Do - Last time I left a to do list, I don't think I did much of it (yet) with the biggest bugaboo being thyroid (still working on it). However I have some very specific ideas in mind now and some of the papers already lined up - here's what I would like to cover next:
Usually people bring other papers to my attention that jump the queue - which is fine by me. But all these papers and subjects are interesting, topical, and will broaden our understanding of all the connections and WHY nutrition is an important piece of the brain environment when one takes a biologic and holistic/scientific approach to maximizing brain health.
Whew. Time to start cleaning the real house - happy Sunday early morning!
1) Contacting me - through the Psychology Today blog and through some comments on this blog I do receive requests for contact. Unfortunately, these requests quickly drop off the top of my email list as I usually think - okay, will get back to that when I have time - and then I don't end up having time! I can tell you I am much, much more likely to answer a specific, narrow question that can be dealt with quickly, or anecdotes about how some aspect of paleolithic/traditional-style diets either worked or didn't work for you (best left in a comment for everyone!). Contacts that sound like you want a full psychiatric consultation will likely not be answered. I would love to help, but can't do a proper job of that without taking a lot of time that I typically do not have. Also, I'm not likely to do that without getting paid, and it's illegal and bad practice to do it (except in certain very specific contexts) in states where I am not licensed. I can't practice medicine over the internet. Typically, the questions are something like: "Have you heard of such and such supplement and what do you think of it? Or "do you know any other psychiatrists who practice like you do in [enter your city here]." The answer is usually no to both questions, for better or worse.
In addition, there are often transference issues and other relationship issues that are very important in psychiatric treatment and questions, and often someone will seek my help because their relationship with their doctor or therapist has something broken - I can tell you right off that I am not the solution in those cases - the best thing to do is to talk to your own doctor or therapist explicitly about the broken part. If a mental health professional doesn't jump on that as a very important and interesting part of your treatment, time to maybe look around for someone else (in your area). Often the most exciting and helpful changes occur after someone tells me how I am not helping them.
2) Comments on Old Posts - There are many fabulous, detailed comments left on old posts, and some with very good questions. If the winds are blowing right, sometimes I have the time to answer them - often I don't. I do generally address questions in comments left in the most recent posts.
3) To Do - Last time I left a to do list, I don't think I did much of it (yet) with the biggest bugaboo being thyroid (still working on it). However I have some very specific ideas in mind now and some of the papers already lined up - here's what I would like to cover next:
a) Diet and violence 2
b) More basic science and genetics/epigenetics of mental health (that is probably a couple of posts - frontal networks, Caspi 2003 paper, etc.) *Dr. K thinks I don't pay enough attention to epigenetics ;-) - I do think about it a lot but don't always address it necessarily, especially in the generational context as I prefer to focus on things we can change, and I can't do anything about what my grandfather ate.
c) Cannabis, psychosis, and COMT genetics
d) Paper Melissa posted on at hunt.gather.love about acne/brain/gut axis.
e) Trace lithium and suicide again, and lithium and dementia.
f) Oxytocin and attachment
g) Frantic, anxious mice and chronic cardio (don't worry, blogblog, I'll try to use a mouse whisperer context)
Usually people bring other papers to my attention that jump the queue - which is fine by me. But all these papers and subjects are interesting, topical, and will broaden our understanding of all the connections and WHY nutrition is an important piece of the brain environment when one takes a biologic and holistic/scientific approach to maximizing brain health.
Whew. Time to start cleaning the real house - happy Sunday early morning!
Subscribe to:
Posts (Atom)