I realize this blog is titled "Evolutionary Psychiatry," and I have yet to actually mention much psychiatry. In part because my job is to stick my nose where it doesn't belong, such asking you about your relationship with your father, or smack in the middle of metabolic syndrome and weight loss. In part we began with the paleolithic theories because I wanted to describe a basis of healthy eating, and put out some more information to say I'm not coming completely out of left field, though some of my perspectives aren't exactly conventional (though perhaps they are exceedingly conventional, seeing as how I prefer to eat as my ancestors did). I'm happy to be proven wrong about my ideas and perspectives if I find something that changes my mind along the way.
But let's talk about depression for a bit. It's a blockbuster, after all. In any given year, approximately 9% of the adult population is suffering from major depression or dysthymia (1). Women are afflicted about 2-3 times as often as men, and 10-15% of women will become depressed after having children.
What is depression? Well, one must have a certain number of the following symptoms for a certain period of time - depressed mood, lack of interest, appetite changes (increased or decreased), sleep changes (increased or decreased), a generally negative outlook, suicidal thoughts, feelings of hopelessness, helplessness, worthlessness, poor energy, poor motivation, poor concentration, feelings of guilt... you get the picture. What causes depression? Well, it isn't zoloft deficiency. (That doesn't mean that zoloft won't help...) But it is obviously a combination of factors, including genetic predisposition, adaptive versus maladaptive coping skills, levels of stress, and sometimes biological or iatrogenic (i.e. caused by other medical treatments) factors.
To appropriately treat depressive disorders, one must obviously address all these these factors, and the generally accepted procedure nowadays is to combine a thorough medical work-up, psychotherapy, and medication if needed. In that respect the treatment for depression is extremely similar to the treatment for obesity and diabetes - which involves medical monitoring, nutritional counseling, psychological counseling if needed, and medication if needed.
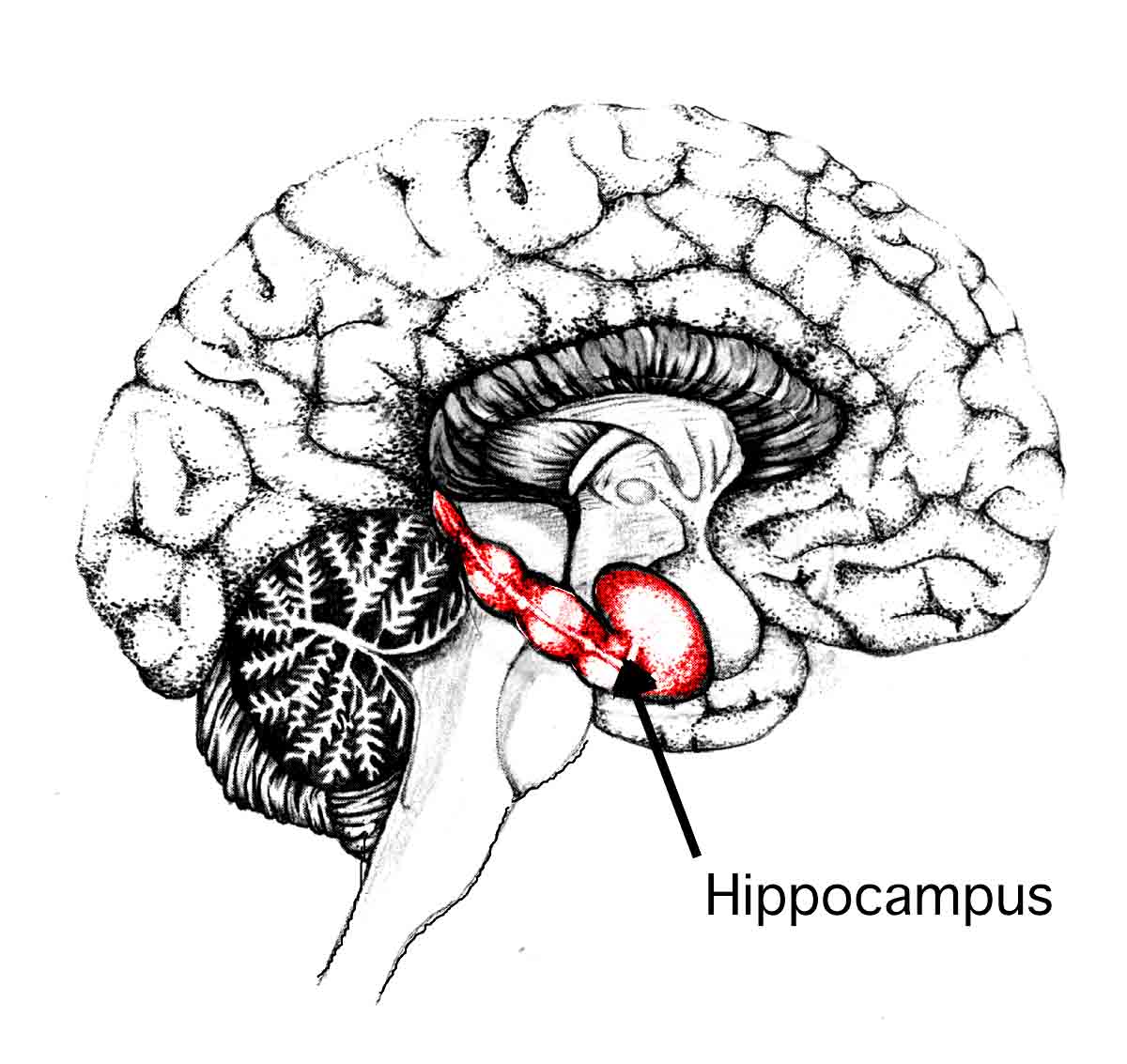
But what *really* causes depression? Biologically speaking? Having a clinical depression means your brain isn't working as it should, and number of factors have been implicated. Among them serotonin system dysfunction, and problems with norepinephrine regulation. But the heart of the matter may be way down in the hippocampus, where stress may interact with genetic predisposition and other factors to create a deficiency in a brain fertilizer of sorts, brain-derived neurotrophic factor (BDNF). It is thought that antidepressant medication actually helps depression by increasing the production of BDNF.
Well, what else can increase BDNF? What other commonly recommended treatment works just as well for depression as antidepressant medication? Exercise, of course. How would exercise increase BDNF in the hippocampus, of all places? There are a number of ways, but the most interesting to me right now is via nitric oxide. Nitric oxide is a gas we make in our red blood cells, especially during exercise and meditative-type breathing. Nitric oxide does all sorts of happy things in our bodies, including relaxing blood vessels and lowering blood pressure, and it is also necessary for erections in men.
Perhaps I have gone far afield of depression at the moment. We psychiatrists, always getting distracted. (Did you know that impotence is related to diabetes and insulin resistance?) But back to the brain! See, antidepressants have to be absorbed in the GI tract, then the active molecules have to somehow make it to the blood brain barrier, and then find the right part of the brain, where a whole cascade of membrane proteins, second messengers, vitamins, and neurotransmitters have to work in concert to increase the production of BDNF to cause the antidepressant effect. Whew. But good old nitric oxide, it is a tiny little molecule, a gas. It doesn't have to rely on all these other players. It can just float through membranes and bind directly to the promoter region of the gene for BDNF, and help the brain make more.
Great! Everyone go out and get some exercise, or meditate. But wait a minute.
It turns out that depressive disorders are a lot more common in people with type II diabetes, and that people with depressive disorders have a 65% greater chance than unaffected adults of developing diabetes. The correlation is so strong, in fact, that for a while researchers were trying to figure out if antidepressant medication actually caused diabetes. (Don't panic - unless the medicine is also making you gain weight, it is probably not adding to your risk of diabetes). As it turns out, successfully treating the depression doesn't improve the increased risk of diabetes. Hmmm, why would that be? Maybe because something else is causing diabetes and the depression, and zoloft isn't FDA-approved to treat insulin resistance?
Well, what does that have to do with the price of tea? I don't know, not 100%. But I have a sneaking suspicion about several factors. Here's one. You see, insulin resistance is associated with endothelial dysfunction (damage to the inner walls of the blood vessels). This means that nitric oxide isn't able to float through the blood vessels (where it is made) into the cells (where it is used). In a nutshell, the nitric oxide of people with insulin resistance cannot do all the things it needs to do. Such as help with sexual activity, reduce blood pressure, and perhaps, just perhaps, help the spectacular brain fertilizer, BDNF, repair the oxidative and inflammatory damage thought to be characteristic of a depressed brain.
So it turns out that maybe it is important for psychiatrist to know a little something about what causes insulin resistance and diabetes, and what an appropriate and effective dietary intervention might be for the whole metabolic derangement in the first place (hint - it's not a high carbohydrate diet).
{kind=link}
Hi - Looks like you have a great blog going here. I went back through your posts, and I am very interested to hear what you have coming up. I am a nutrition and exercise science student who is very interested in evolutionary medicine, especially evolutionary psychiatry.
ReplyDeleteI have been reading whole health source, nephropal, animalpharm, panu, heartscan, hyperlipid, etc for a couple years and am always trying to tie this information in with psychology as well. I'm looking forward to your posts.
Have you read the section on depression by Chris at the healthy skeptic? He's pretty on point with his stuff and I'm wondering what your thoughts on his work are...
Tyler
Fantastic blog. Will be adding this to my regularly followed blogs. I love your approach - very similar to mine as a nutritionist. It is unbelievable the number of people I see who have insulin resistance, don't exercise, and are 'depressed'. I think I'd be depressed too if I treated my body the same way these people do.
ReplyDeleteIf you get the chance, have a look at some of the work that's about looking at gastrointestinal health and anxiety states. Very interesting.
Keep up the awesome posting.
Hi Tyler -
ReplyDeleteI agree wholeheartedly with most of what Chris says over at The Healthy Skeptic, except on two points, antidepressants (I believe they are neuroprotective, not toxic, and when used thoughtfully and with appropriate expectations they can make a very positive difference, but they are definitely not the end-all, be-all in the treatment of depressive disorders, by any means), and St. John's Wort (it works well, and I wish I could recommend it, but Hypericum perforatum is apparently very difficult to harvest in a way that the dose in the pills from month to month will be anywhere near the same - Consumer Reports - I believe, I'm not 100% sure it was them - tested the same brands through a year and the dosages in the same brand pills were incredibly different, and not what was on the label. It is also most likely an MAOI, and the drug interactions are extreme.) SAM-E is a good antidepressant, too, and much easier to get an appropriate, consistent dose, and good for the liver!
Hi Jamie - thanks for adding me to your list. GI/mood/anxiety stuff is definitely coming up!
Hi Dr. Dean,
ReplyDeleteI just wanted to congratulate you on your fine blog. Interesting concept, linking psychiatry and Evolutionary medicine. But it is all connected isn't it? You get it, that is why we at nephropal.com have made our big policy change. We finally came to understand that in order for one to be a complete physician the next step has to be taken, which is to become qualified in Evolutionary Medicine. We hope to be up and running soon with our Evolutionary Medicine Society which will offer CME credit courses along with certification in evolutionary Medicine. You are exactly what evolutionary Medicine medicine needs. We are going to focus on MD's, DO's, and PA's.
You do get us. we look forward to a long association with you. I would like to extend an invitation to you to be a guest commenter at your convenience. I think that our readers would be very interested in your take on Psychiatry and Evolutionary Medicine combined. You have a great site. Let us know what you think of this idea. Good luck.
Billy E
Nephropal.com
Billy E. - I'd be honored.
ReplyDeleteEmily