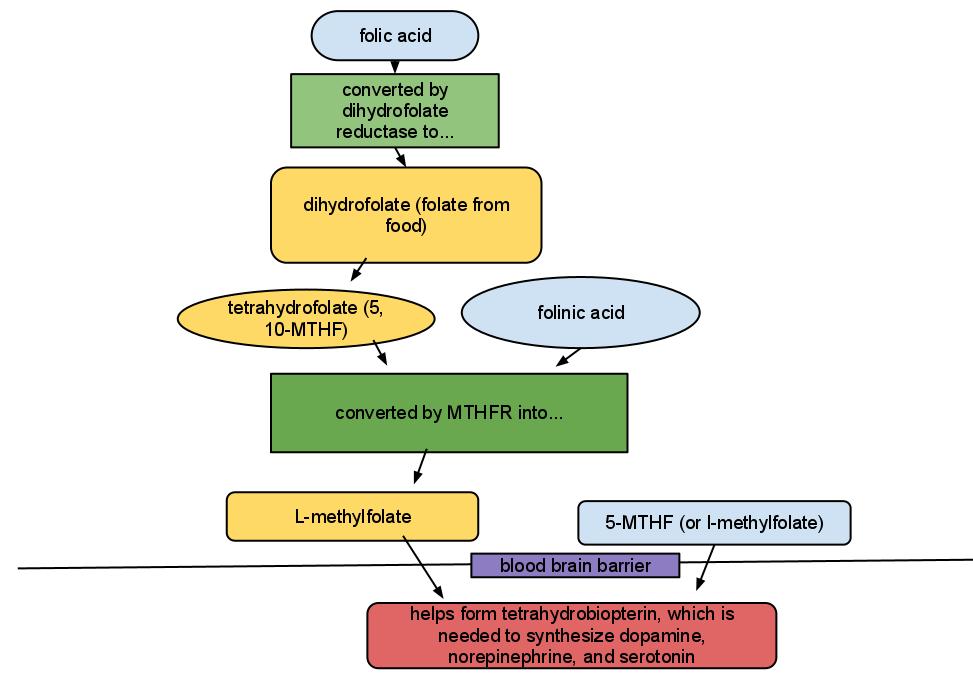
Let's just start with a diagram, and an explanation for those of us who were taught some basic organic chemistry. Folate does not equal folic acid. I know. It's weird. For all the other acids, -ate equals -ic acid (such as phytate and phytic acid), but for whatever reason, folate = dihydrofolate, and folic acid equals synthetic folate that is used to fortify foods in the US and in multivitamins. Let me supply you with a handy diagram:
 | ||
|
Now why would a psychiatrist care about this pathway? Well, folks with depression have increased risk of having crappy dihydrofolate reductase activity (meaning they have a hard time turning synthetic folic acid into dihydrofolate - this enzyme is also inhibited by the medication lamotrigine). In addition, folks with depression are more likely to have issues with the MTHFR enzyme (I know - it stands for methylenetetrahydrofolate reductase but that's not what I call it in my head either). So if you prescribe medications meant to maximize the efficiency of neurotransmitter* transmission in order to treat depression or anxiety, or if you just want nature to maximize the efficiency of neurotransmitter transmission (which everyone would agree is preferable, if possible), you want plentiful tetrahydrobiopterin in the brain.
You can see from the diagram that cheap, plentiful folic acid may not aways become the final active product in the brain. You can also see that expensive, prescription 5-MTHF (deplin) might be useful for some people, though you may be annoyed if you know that deplin has never been tested head to head against folic acid.
5-MTHF and folinic acid have had some decent studies increasing response rates to antidepressant therapies, and decreasing cognitive symptoms of depression. The results for folic acid supplementation itself have been mixed. And, given some genetic polymorphisms (such as C677T, affecting the MTHFR gene), a peripheral folate level (which I have drawn routinely) will not necessarily tell us about folate levels in the brain.
But why not just pour tons of folic acid into the system - well folic acid has some risks. For one, it has been shown to mask some of the first symptoms of B12 deficiency (which I have seen - none of my patients with low B12 have had the classic hemotologic signs that doctors have long relied upon to help diagnose B12 deficiency - possibly because folic acid supplementation is now abundant in the food system). In addition, folate is a growth factor, and one has to be careful about pouring growth factors into the system, lest one risk cancer - the risk of colorectal cancer being the most studied and the most likely (1) caused by widespread folic acid supplementation. (The results of the epidemiological studies are mixed however, with this large US study showing no correlation).
Now, if you take a ton of folic acid (more than 800 mcg daily - 800 mcg being the normal dose in prenatal vitamins), it has been shown that the excess folic acid won't be metabolized, and that excess folic acid in the serum actually reduces the amount of l-methylfolate that reaches the brain, with a potential increase in depression. Supplementation with l-methylfolate will not mask B12 deficiency and is less likely to be a risk for colon cancer (since the upstream agent, folinic acid, is used to kill cancer). But… the cost. A thirty day supply of deplin can cost as much as $80 at the pharmacy, and the cheapest I have found it is $70 for a 3 month supply direct from the manufacturer. As a "medical food" it is not covered by insurance. And yes, in my clinical experience, I have some patients who have not responded to folic acid supplementation who have done very well on deplin.
Folate, real, natural happy dihydrofolate from food is most plentiful in leafy green vegetables, fruits, and (ahem) legumes. Cereals and grains are fortified with synthetic folic acid.
Hopefully this article will clarify some things… or maybe we will consume few more leafy green veggies and fruit along the way...
*serotonin, dopamine, and norepinephrine are neurotransmitters
Fava, M and Mischoulon, D. Folate in Depression: Efficacy, Safety, Differences in Formulations, and Clinical Issues. J Clin Psychiatry 2009;70[suppl 5]:12-17
Frankenburg, FR, Folate supplementation: is it safe and effective? (letter) J Clin Psychiatry. 2008;69(9):1352-1353