Young the Giant. Cough Syrup (right click to open in new tab)
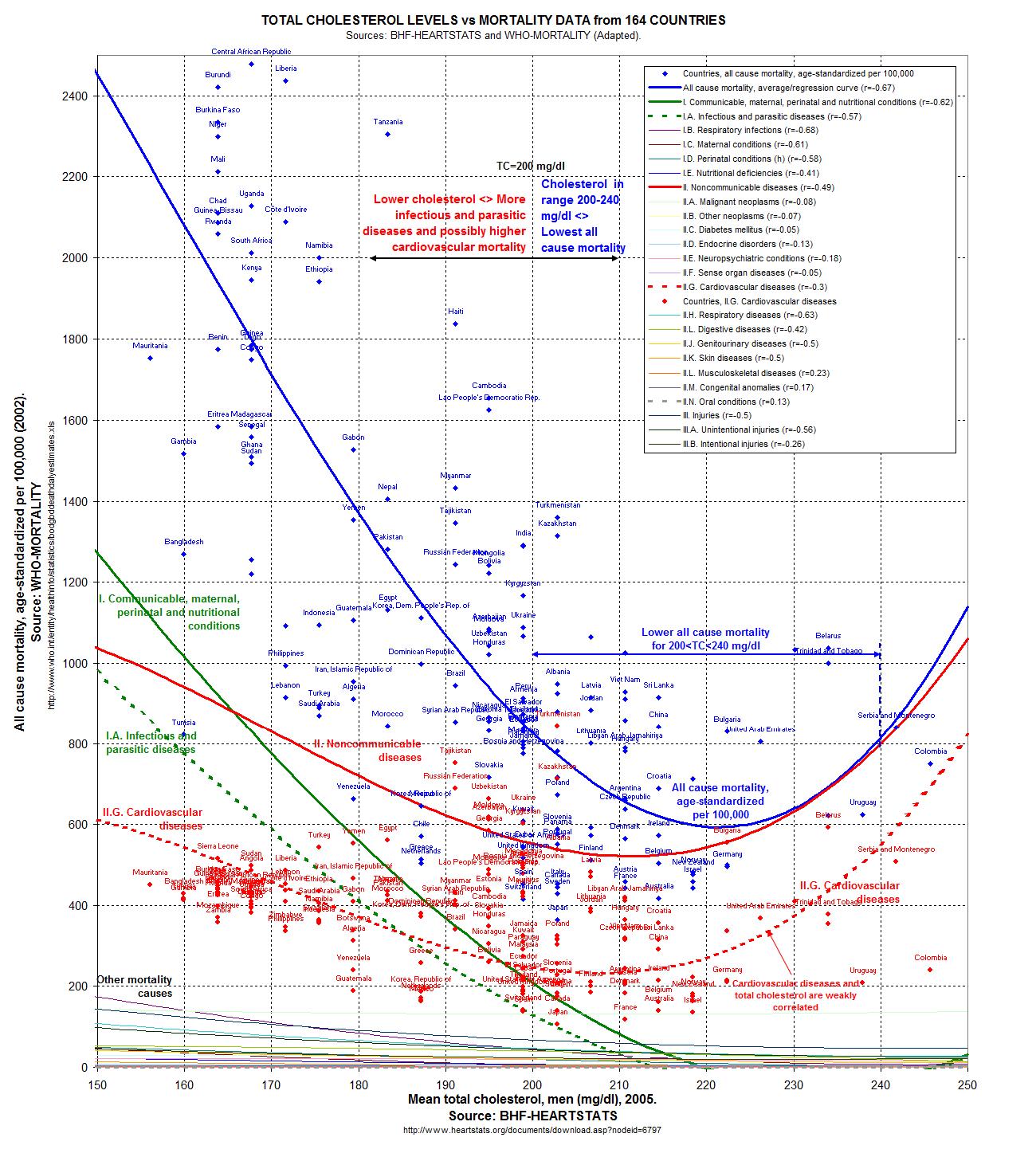
My thoughts are in response to a culmination of a number of recent news items in medicine. First, at the end of 2011, an expert panel convened by the National Heart, Lung, and Blood Institute recommended universal lipid screening in children 9-11 years of age and again at 17-21 years of age. On surface this seems innocuous enough… from a conventional medicine standpoint when one considers cholesterol to be an important marker of health. (Let's ignore for a little bit the fact that low cholesterol (along with exceptionally high) is associated with increased overall mortality in study after study after study.) No matter what, one of the most basic tenets of modern medicine is to consider the point of the test. If one runs a test, one must be prepared to do something with the information. If you aren't going to do anything about it, then why run the test in the first place?
{kind=link}
I was pleasantly surprised by a JAMA editorial from earlier this month concerning these universal recommendations. The new NHLBI guidelines are linked to recommendations about both behavioral and drug therapies. The behavioral therapies are obvious -- increased exercise and a prudent diet (*cough*). And surely we should be recommending a diet focused on healthy, whole foods and avoiding processed foods for everyone. Healthy activity is also a universal and without too much controversy. But then you get to drug therapy for dyslipidemia, which in 2012 means statins for kids.
Here is where the JAMA editorial gets real. They note that in a meta-analysis of 10 primary prevention trials (primary prevention refers to people without prior cardiovascular disease, more or less the general population, whereas secondary prevention refers to drug treatment of folks who have already had a heart attack or stroke), statin use was associated with a 30% reduction in coronary events and a 12% reduction in total mortality (1). (Let's ignore the fact that these are relative risk rather than absolute risk numbers for now, more on that later!) Let's not ignore the fact that atherosclerosis begins in childhood, and that cholesterol levels track from childhood to adulthood. Reducing LDL cholesterol levels appears to extend the life of people with familial hypercholesterolemia.
But. But but but but but. Even a cardiologist would have to agree that most children with "dyslipidemia" will not develop early heart disease. Treating these children with statins exposes them to unwarranted risk and side effects. Drugs that lower cholesterol, such as fibrates, sterols, or the newer CETP inhibitors, are only associated with an increased or unchanged risk in cardiovascular events, suggesting that lowering cholesterol numbers itself is not a means to an end. The studies for the first CETP inhibitor, torcetrapib (which does a crackerjack job of lowering LDL and raising HDL at the same time! Whee!) showed a modest increased hazard ratio (only 1.25) which scarily enough would not have been detected if only the cholesterol measures were used, rather than overall mortality or cardiovascular events in the initial studies.
The JAMA authors go on to remark that statins have been tested in small numbers of children ( a few hundred, for studies ranging from 8 weeks to 2 years) for brief periods of time, and only the surrogate outcomes (cholesterol measures) have been assessed. So far, trials have lacked the size and duration to demonstrate any health benefits for children. If there are long term harms, it is unclear how these might be detected. Surely this uncertainly would be enough to give most pediatricians pause, to say the least.
So if one screens, there will be a compulsion to act quickly on the results. Do you give statins to children with NO data? Wouldn't you recommend whole foods, avoiding processed garbage and prudent exercise as staples for all children as a matter of course? "What this novel public health intervention in children clearly lacks is an evaluation to determine whether the long-term risk-benefit profile may in fact be favorable or harmful."
Let's move on from children to women, where statin use has also been controversial, as a very new meta-analysis was published in the Journal of the American College of Cardiology this very week: Meta-Analysis of Statin Effects in Women Versus Men. I imagine this study will be used in order to further pressure all of us with average cholesterol to go on medicine for primary prevention of heart disease. This meta-analysis (which brings together the data from a number of different studies) strives to do what no statin study has done before--prove any benefit in women, particularly in primary prevention. In the end the authors find in a compilation of data from 18 trials with sex-specific outcomes (141,235 people and 40,275 women) that outcomes were similar for women as for men. That is a statistically significant benefit for women as well as men of similar magnitude in both primary and secondary prevention. All-cause mortality was also lower with statin therapy both in women and in men with no significant differences between the sexes.
Well. Hallelujah. At last. The conclusion: "Statin therapy should be used in appropriate patients without regard to sex."
Of course, as we all know, the devil is in the details. And in a beautiful editorial in the very same edition of Journal of the American College of Cardiology we have "Controversy and Consensus About Statin Use: It Is Not About the Sex." The editorial says, yes, indeed, finally, and it is no surprise, that statin therapy should be of similar benefit to women and men, but what does that mean, exactly?
It means, with secondary prevention, those who have already had a heart attack for example, that statins do indeed impart benefit, and I'm willing to extend that benefit to women as well as men. But when we come to primary prevention (statins in people with risk factors for heart disease, not proven heart disease), we are talking a whole different kettle of fish.
First off, of more than 2300 studies identified by the doctors doing the meta-analysis, only 18 met all the inclusion criteria (meaning they were of high quality enough to be included). 8 were primary prevention trials, and 17 were funded by the pharmaceutical industry, and only 2 included sex-specific data on side effects (or "adverse events"). One of the included trials was JUPITER, which remains controversial as it was halted early and had a short follow-up.
The "devil" here is that women are considerably less likely to die of heart disease than are men. Thus any primary prevention in women will need to meet a more stringent requirement than in men, as by numbers alone primary prevention of heart disease will be of lesser benefit in women. The risks of diabetes, muscle problems, cognitive deficits, and perhaps increase in cancer would be expected to be more of an issue in women, with smaller lean mass thus higher relative statin dose (same issue is at play in children), longer lifespans and lower risk of heart disease and higher risk of cancer than men. While "relative risk" of decrease in heart disease (say a decrease of 2% to 1%, with a relative risk decrease of 100%!) might be promising, the absolute risk (that change from 2 to 1%) is unimportant. So here we get to the heart of the matter:
Women without CVD have lower annual mortality risk and lower CVD risk than men without CVD. Therefore, the absolute benefit of statins will typically be less for women than men, suggesting it might be appropriate that women receive statins less frequently than men in the setting of primary prevention. The current meta-analysis provides information about sex-specific relative risk benefit and not absolute benefit. Both absolute risk of CVD and the proportionate risk reduction associated with statin therapy are needed to make informed clinical choices with regard to the use of statins for primary prevention. Although the latter might be similar for the sexes, the former might be quite different.As only 2 studies provided sex-specific risk data, we simply cannot evaluate the risk of statins for primary prevention in women Adverse outcomes are extremely clinically important when we are giving medicines to healthy people to prevent disease. More wisdom from the editorial:
Sex-specific results in cardiovascular prevention tirals should be provided for relative and absolute benefits, adverse outcomes, and cost-effectiveness. Only then we will know with less uncertainty whether what is good for the gander is also good for the goose. Medicine is still an art. [emphasis mine]And, finally, some thoughts on some email conversations I've had with Kurt Harris on low dose naltrexone. We were discussing the use of LDN in allergy and autoimmune disease, and I had stumbled upon this skeptical webpost: Low Dose Naltrexone, Bogus or Cutting Edge Science? The truth is that LDN has shown a robust benefit for a very challenging illness, Crohns Disease, in studies at Penn State (2). In these studies, the inexpensive and by any rational observation low risk low-dose naltrexone performed better than the incredibly expensive noxious anti-TNF-alpha Humira. We certainly know much more about Humira's risks-- they are many, and yet it is somehow dangerous and "woo" to recommend a trial of LDN in comparison. LDN has real potential to modify the immune system to decrease deadly and intolerable immune reactions in diseases such as Crohns. Naltrexone has been in use for a decade or more, and while there is a dose-dependent risk of liver damage, that risk tends to happen at 150mg daily. LDN is about 4.5 mg a day. Sure, there is no argument that we should have more data, but how is it crazy and dangerous to recommend LDN for Chrons (as opposed to Humira or even steroids) and not crazy and dangerous to recommend statins for primary prevention, a very accepted practice?
In my mind, when we are considering difficult illnesses with only dangerous evidenced-based cures, we have consider common sense and the cost of large trials and the corrupt influence of money and the pharmaceutical industry. One such example is the vitamin supplement SAMe, which performed better in trials at MGH than any FDA approved adjunctive treatment for resistant depression. SAMe is not without risks (mania and elevated homocysteine), yet surely Abilify (which has FDA approval), 10X more expensive and with risks of permanent movement disorders, weight gain, metabolic syndrome, and diabetes should sensibly be a second-tier option in resistant depression compared to SAMe, with a decades-long track record of randomized controlled trials? Somehow that is not the case. Somehow we put Abilify ahead of the mere supplement.
I'm preaching to the choir. But I suppose that is what a blog is for. The papers march on, the money, the meta-analyses, the editorials. Does anyone demonstrate common sense in actual clinical practice? We shall have to see. Money (and time?) is running out for us to come to our senses.
(I read recently The Cholesterol Delusion by Ernest Curtis, M.D., a cardiologist, at the recommendation of Mike Eades. It's a short read, pointed, and interesting. Worth the time. One of his most important points of wisdom is that any study or news report touting relative risk in lieu of absolute risk has an agenda and is trying to make a dramatic statement when there may or may not be any reasonable difference in risk.)
well, friend. when you get right down to it and ask yourself what it is we do in this profession of ours and what the actual benefit is, it can be a bit depressing. recently spent time taking care of someone who spent 4 days at home having an mi, then came in. discovering the complete failure of his ventricle he was transferred to our service (we of course being the university hospital) where we uncorked all the big tech (percutaneous ventricular assist devices, fancy vent strategies, nitric oxide, etc, etc) and of course nothing will work cuz when you have 2 dead ventricles and aren't a transplant candidate then....
ReplyDeletedid the same with some ecmo recently.....
why no one ever asks, ummm. why exactly is this young person 400 pounds.
amazing how many laugh at my dietary talks.
had the pharmacist and residents point out several times last week that our patients (post CABG) weren't on their home doses (80mg atorvastatin) of meds. i found it necessary to point out that apparently said doses and meds didn't seem to be producing a benefit ....crickets
am rather close to going out on my own, starting a gym/primary care clinic/training program. i'm ready to take care of people interested in taking care of themselves.
statins for kids. christ.
These problems are clearly driven by greed. They are absolutely effects of greed and profit seeking and any other interpretation is naive, rose colored glasses or willful ignorance to truth.
ReplyDeleteWhen it so happens that every stupid therapy/protocol in medicine happens to fill someone's pockets with piles and piles of gold (e.g. giving abilify to everyone/thing, but ignoring SAMe or any other supplement) you can't attribute that to medicine being an imperfect science, or an art. At that point, when we clearly see "stupid therapies" correlating 100% with "lots and lots of profits for someone/people" then we see it isn't an oversight, a mistake, but purposeful deception done for greed and greed alone.
re: LDN... Wonder if helminthic therapy would be safer and just as effective...
ReplyDeleteEffective, perhaps, but ewww... I'd rather take the naltrexone.
DeleteDan’s comments above are most telling. Unless you are on the drug side of medicine who would want to enter or remain in this field once you have seen the “light” so aptly described by the many MD’s, PhD’s, VDM’s and just plain bright people who belong to this “choir”?
ReplyDeleteOnce you have seen the truth and speak about it you are immediately marginalized or seek to marginalize yourself.
I think about young doctors. What if they have entered medicine knowing the truth or see the truth early in their career. How will they view their future in medicine? Eventually they will be expected to prescribe stains or some other drugs they know are useless and/or harmful. If governments / drug companies (they are hand in hand at this point) have their way, they will be prescribing these drugs to children.
Perhaps the blogosphere is the agent of change here – I hope so. Otherwise....
Phil
Dan, you should have a blog, man. From the front lines. And yes, what are we doing? I spend a lot of my time cleaning up huge piles of stinking mess created by very well-meaning people (and sometimes those messes are my own!). This very morning, young person came in on 5 different meds, three of which could interact and cause a deadly heart rhythm (unlikely but certainly possible), another three of which could interact and cause seizures (also unlikely but possible.) It is awfully easy to have 20/20 hindsight but, seriously…
ReplyDeleteWoo: to be fair I think we need to add in ignorance, stupidity, and good intentions.
Js290: Helminthic therapy is much more expensive. Everything I've seen and heard about it would make me suspect it could be extremely effective.
Thackray: As a psychiatrist I am already somewhat marginalized and I'm allowed (perhaps even expected) to be a bit of a kook. We are managed to some extent but not so much as the primary care doctors, who are more and more getting graded and even paid by how closely they adhere to evidenced based guidelines (having diabetics and other high risk folks on certain meds, following up with certain frequency, etc.,). But I am unclear of the future. I'm hopeful these critical editorials from JAMA and JACC mean that caution about these prescriptions is swinging back into vogue.
I wonder if y'all can fully appreciate how healing it is for us lay folk to hear MDs admitting to a systemic problem within institutional medicine.
ReplyDeleteTHANK YOU
@Js
ReplyDelete"Wonder if helminthic therapy would be safer and just as effective..."
The remission rates for Crohns in the penn LDN trial and in Weinstocks TSO trial at Iowa were fairly similar and both seemed to be very effective for that disease. It is very impressive that the penn trial documented remission with endoscopy as well as by symptoms.
TSO is very expensive - requiring the maintenance of live pigs for harvesting and counting the ova to give to the patients. Since TS is not a human pathogen, it must be taken regularly. TSO treatment commonly causes GI side effects, and essentially induces a mild eosinophilic enteritis of the colon. Hookworm infection is not FDA approved and this definitely causes an enteritis which can also be symptomatic. FInally, infection with TT, or human whipworm, apparently can actually make allergies WORSE before they get better, when given for IBD.
The bottom line is that it is remarkable how similar the efficacy is between LDN and TSO treatment for Crohn's and the putative mechanism of LDN may induce similar cytokine and cellular regulatory responses to worm infection or pseudo-infection with TSO.
Yet LDN seems to have much fewer side effects, is easily obtainable off label, and can be as cheap as $6 a month to take if you do your own home compounding. LDN also has some theoretical side effects that could be highly beneficial, like suppression of proliferation of cancer cells.
I don't think LDN will cure everything and anything, but its use as an immune modulator for any disease that seems to be related to failure to suppress Th1 or TH2 responses deserves to be considered further.
@P Flooers
ReplyDeleteI hope you appreciate that none of what I have written is particularly controversial or outside the bounds of normal conversation and debate in discussing these recommendations. Both the editorials I mentioned were published in hugely mainstream journals. Somehow the consensus guidelines have become the voice of the fringe.
Thanks for opening that up to me. I really appreciate the discussion.
ReplyDeleteI was just reading the new insights to grehlin and the hypothalmic ovarian brain gut axis. I have a feeling that it explains the bipolar one sequence. What kind of doctor would explore the grehlin effect on the growth hormones/vagus nerve and treat that way? I realize lithium is nearly impossible to get off of, but if all the right things were measured and corrected, along with sleep and good health, it might be possible. It sure seems worth exploring.
ReplyDelete