Another one for the marine-derived highly unsaturated fatty acids are probably really important for proper brain function files: This new paper has been tweeted quite a bit lately: Suicide Deaths of Active Duty US Military and Omega-3 Fatty Acid Status: A Case-Control Comparison
It is an observational study, but large for a suicide study (suicide is, fortunately, quite rare). All told, 800 randomly selected suicide victims in the armed services were selected between 2002-2008, and compared to 800 matched controls. Cases were matched for time and theater of deployment, exposure to stress during deployment, report of mental health status, and demographics among other data points. (Though later the paper says 99.1% of the controls had been deployed vs. only 61.9% of the suicides, so the deployment location and duration were not added as covariates to the end calculations).
So, fatty acid of the blood of the participants - in short, the lower the DHA in the blood, the more likely the person was to have committed suicide. The relationship was linear and true of all octiles studied. There were only 70 women in the samples, and they tended to have higher DHA levels than the men, and lower suicides (among women, the omega 3 status to suicide relationship was not statistically significant as it was clearly so among the men). Men in the lowest DHA octile were 62% more likely to commit suicide than those in the highest octile.
Other fatty acids of interest - lower levels of stearic acid (saturated! My goodness! Found in chocolate! And steak!) were found to be associated with increased risk of suicide (my preliminary conclusion - eat more chocolate - though it is only observational - I'll risk it and eat your chocolate if you are uncertain). Also, higher palmitoleic acid (a monounsaturated acid made from the saturated palmitic acid) levels correlated with a lower level of suicide risk.
In this study, US military personnel were found to have, on average, a lower DHA level than average North American, Australian, Mediterranean, and Asian populations (unlike the medical students I wrote about a few articles ago, who had higher levels than the general population). In fact, among Chinese suicide attempters, nearly all of them had higher levels of omega 3 DHA than the highest octile of the US military personnel studied. And when both populations were studied together, the lowest DHA levels coincided with a 5-6 fold increased risk of suicide. For perspective, this risk increase coincides with the risk of undergoing severe stress under deployment (seeing wounded, killed, or dead comrades, for example) and the risk of suicide.
We can't determine causality, but common sense and and evolutionary perspective should surely make us suspicious - eat those marine omega3s and keep your 6:3 ratio minimal. The paper recommends 2 grams daily of marine omega 3s.. Seems reasonable.
Tuesday, August 30, 2011
Saturday, August 27, 2011
Folate! The Beginning.
Did I ever mention that I'm not a big fan of the folate cycle? Not because it's not important, but because it is intensive, poorly understood, and hard to remember. Probably a bad reason to dislike it, as far as those things go…
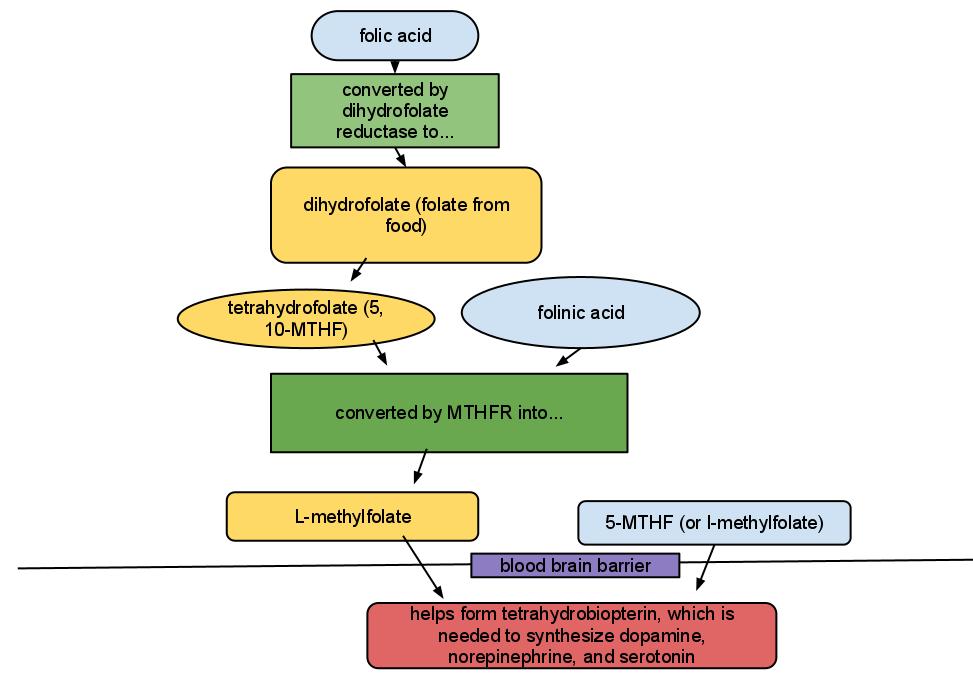
Let's just start with a diagram, and an explanation for those of us who were taught some basic organic chemistry. Folate does not equal folic acid. I know. It's weird. For all the other acids, -ate equals -ic acid (such as phytate and phytic acid), but for whatever reason, folate = dihydrofolate, and folic acid equals synthetic folate that is used to fortify foods in the US and in multivitamins. Let me supply you with a handy diagram:
Now why would a psychiatrist care about this pathway? Well, folks with depression have increased risk of having crappy dihydrofolate reductase activity (meaning they have a hard time turning synthetic folic acid into dihydrofolate - this enzyme is also inhibited by the medication lamotrigine). In addition, folks with depression are more likely to have issues with the MTHFR enzyme (I know - it stands for methylenetetrahydrofolate reductase but that's not what I call it in my head either). So if you prescribe medications meant to maximize the efficiency of neurotransmitter* transmission in order to treat depression or anxiety, or if you just want nature to maximize the efficiency of neurotransmitter transmission (which everyone would agree is preferable, if possible), you want plentiful tetrahydrobiopterin in the brain.
You can see from the diagram that cheap, plentiful folic acid may not aways become the final active product in the brain. You can also see that expensive, prescription 5-MTHF (deplin) might be useful for some people, though you may be annoyed if you know that deplin has never been tested head to head against folic acid.
5-MTHF and folinic acid have had some decent studies increasing response rates to antidepressant therapies, and decreasing cognitive symptoms of depression. The results for folic acid supplementation itself have been mixed. And, given some genetic polymorphisms (such as C677T, affecting the MTHFR gene), a peripheral folate level (which I have drawn routinely) will not necessarily tell us about folate levels in the brain.
But why not just pour tons of folic acid into the system - well folic acid has some risks. For one, it has been shown to mask some of the first symptoms of B12 deficiency (which I have seen - none of my patients with low B12 have had the classic hemotologic signs that doctors have long relied upon to help diagnose B12 deficiency - possibly because folic acid supplementation is now abundant in the food system). In addition, folate is a growth factor, and one has to be careful about pouring growth factors into the system, lest one risk cancer - the risk of colorectal cancer being the most studied and the most likely (1) caused by widespread folic acid supplementation. (The results of the epidemiological studies are mixed however, with this large US study showing no correlation).
Now, if you take a ton of folic acid (more than 800 mcg daily - 800 mcg being the normal dose in prenatal vitamins), it has been shown that the excess folic acid won't be metabolized, and that excess folic acid in the serum actually reduces the amount of l-methylfolate that reaches the brain, with a potential increase in depression. Supplementation with l-methylfolate will not mask B12 deficiency and is less likely to be a risk for colon cancer (since the upstream agent, folinic acid, is used to kill cancer). But… the cost. A thirty day supply of deplin can cost as much as $80 at the pharmacy, and the cheapest I have found it is $70 for a 3 month supply direct from the manufacturer. As a "medical food" it is not covered by insurance. And yes, in my clinical experience, I have some patients who have not responded to folic acid supplementation who have done very well on deplin.
Folate, real, natural happy dihydrofolate from food is most plentiful in leafy green vegetables, fruits, and (ahem) legumes. Cereals and grains are fortified with synthetic folic acid.
Hopefully this article will clarify some things… or maybe we will consume few more leafy green veggies and fruit along the way...
*serotonin, dopamine, and norepinephrine are neurotransmitters
Fava, M and Mischoulon, D. Folate in Depression: Efficacy, Safety, Differences in Formulations, and Clinical Issues. J Clin Psychiatry 2009;70[suppl 5]:12-17
Frankenburg, FR, Folate supplementation: is it safe and effective? (letter) J Clin Psychiatry. 2008;69(9):1352-1353
Let's just start with a diagram, and an explanation for those of us who were taught some basic organic chemistry. Folate does not equal folic acid. I know. It's weird. For all the other acids, -ate equals -ic acid (such as phytate and phytic acid), but for whatever reason, folate = dihydrofolate, and folic acid equals synthetic folate that is used to fortify foods in the US and in multivitamins. Let me supply you with a handy diagram:
 | ||
|
Now why would a psychiatrist care about this pathway? Well, folks with depression have increased risk of having crappy dihydrofolate reductase activity (meaning they have a hard time turning synthetic folic acid into dihydrofolate - this enzyme is also inhibited by the medication lamotrigine). In addition, folks with depression are more likely to have issues with the MTHFR enzyme (I know - it stands for methylenetetrahydrofolate reductase but that's not what I call it in my head either). So if you prescribe medications meant to maximize the efficiency of neurotransmitter* transmission in order to treat depression or anxiety, or if you just want nature to maximize the efficiency of neurotransmitter transmission (which everyone would agree is preferable, if possible), you want plentiful tetrahydrobiopterin in the brain.
You can see from the diagram that cheap, plentiful folic acid may not aways become the final active product in the brain. You can also see that expensive, prescription 5-MTHF (deplin) might be useful for some people, though you may be annoyed if you know that deplin has never been tested head to head against folic acid.
5-MTHF and folinic acid have had some decent studies increasing response rates to antidepressant therapies, and decreasing cognitive symptoms of depression. The results for folic acid supplementation itself have been mixed. And, given some genetic polymorphisms (such as C677T, affecting the MTHFR gene), a peripheral folate level (which I have drawn routinely) will not necessarily tell us about folate levels in the brain.
But why not just pour tons of folic acid into the system - well folic acid has some risks. For one, it has been shown to mask some of the first symptoms of B12 deficiency (which I have seen - none of my patients with low B12 have had the classic hemotologic signs that doctors have long relied upon to help diagnose B12 deficiency - possibly because folic acid supplementation is now abundant in the food system). In addition, folate is a growth factor, and one has to be careful about pouring growth factors into the system, lest one risk cancer - the risk of colorectal cancer being the most studied and the most likely (1) caused by widespread folic acid supplementation. (The results of the epidemiological studies are mixed however, with this large US study showing no correlation).
Now, if you take a ton of folic acid (more than 800 mcg daily - 800 mcg being the normal dose in prenatal vitamins), it has been shown that the excess folic acid won't be metabolized, and that excess folic acid in the serum actually reduces the amount of l-methylfolate that reaches the brain, with a potential increase in depression. Supplementation with l-methylfolate will not mask B12 deficiency and is less likely to be a risk for colon cancer (since the upstream agent, folinic acid, is used to kill cancer). But… the cost. A thirty day supply of deplin can cost as much as $80 at the pharmacy, and the cheapest I have found it is $70 for a 3 month supply direct from the manufacturer. As a "medical food" it is not covered by insurance. And yes, in my clinical experience, I have some patients who have not responded to folic acid supplementation who have done very well on deplin.
Folate, real, natural happy dihydrofolate from food is most plentiful in leafy green vegetables, fruits, and (ahem) legumes. Cereals and grains are fortified with synthetic folic acid.
Hopefully this article will clarify some things… or maybe we will consume few more leafy green veggies and fruit along the way...
*serotonin, dopamine, and norepinephrine are neurotransmitters
Fava, M and Mischoulon, D. Folate in Depression: Efficacy, Safety, Differences in Formulations, and Clinical Issues. J Clin Psychiatry 2009;70[suppl 5]:12-17
Frankenburg, FR, Folate supplementation: is it safe and effective? (letter) J Clin Psychiatry. 2008;69(9):1352-1353
Friday, August 26, 2011
More About Thiamine
Some of the most harrowing stories of nutrient deficiencies come from the 18th and 19th century British Navy. Perhaps because the officers on the long voyages had nothing better to do than document the slow, desperate and horrific progression? Recently there was a PBS special on the Erebus, a ship that left Britain in 1845 under Captain Franklin to look for the Northwest Passage. This voyage occurred during a century of Arctic and Antarctic exploration that included Shackleton's famous doomed voyage (the memoir, South, is well worth reading). Those poor sailors on the Erebus, though. See, just before their planned expedition, the process of food canning was, um, perfected. The Admiralty was thrilled - now they could send the ships around the world and not worry about local conditions or foraging for food. They would include plenty of canned fruits rich in vitamin C so that most horrible sailor's disease, scurvy, would not affect the crew. Scurvy is a horrible way to die - your connective tissue degrades and you spend a great deal of time in terrible pain as you slowly bleed to death internally. Go civilization! Let's conquer the Arctic!
Well, the ship sailed off with Franklin and a crew of 128 and was nearly never heard from again. There were a few accounts of sightings, and rumors of mutiny and cannibalism reached Britain. Turns out that the cans were soldered with lead, and the water supply may also have been contaminated. And it so happens that the vitamin C in canned foods only lasts about a year, so after the ship bogged down in ice for several seasons, the sailors who weren't weakened, crazed, and killed by lead poisoning succumbed to hypothermia and scurvy. The luckier sailors on the Shackleton expedition brought some guns along and hunted and fished for the years they were stranded after their ship was crushed in the ice (one can't help but notice that all those cute sled dogs present at the beginning of the voyage are gone by the end). And they got through okay - Shackleton didn't lose a single man. The crew of the Erebus may be some of the first victims of modern processed food.
While thiamine deficiency was described as "sailor's asthma" in the Navy, this disease was better known in Japan as "Kakke" and had been described as early as year 808 (1). In the early 20th century, 30 per 100 Japanese died of the disease. Once thiamine was discovered, mortality dropped to 0.5 per 100 Japanese. The major symptoms were poor reflexes, swelling, low diastolic blood pressure, and tender calf muscles. Cardiovascular symptoms include a weakening and enlargement of the heart, called "cardiomyopathy" which will eventually result in heart failure (and lung symptoms as the circulation backs up in the lungs - thus "sailor's asthma.") Peak deaths, both in adults and infants, occurred between August and September, even more so when humidity was high.
Before thiamine was isolated, it became obvious (from voyages of the Japanese Navy and from birds fed a strict diet of white rice) that polished rice was the major contributor to beriberi, and that adding red beans, dried meat, rice bran, or barley to sailor's rations prevented the disease. It is the original "empty calorie" disease. Thiamine, first isolated in 1926, is now known to have some plentiful sources: meat, wheat germ, liver, organ meats, poultry, eggs, fish, beans, nuts, and whole grains. Cooking and processing depletes the vitamin, but you don't need much - just 0.5mg per 1000 calories consumed. Polyphenols in coffee and tea can inactivate thiamine, so stick to red wine (just kidding - alcohol interferes with the absorption of thiamine, remember?)
Like most vitamins, thiamine is taken up into the body and then immediately modified into a number of derivatives. The most famous is thiamine diphosphate (also known as TPP) - this thiamine is the one that plays a part in a bunch of energetic reactions in glucose metabolism. If you want your citric acid cycle to run (and believe me, you do), you need thiamine diphosphate. Bodybuilders and BCAA chuggers take note - you also need TPP to decarboxylate the keto acids derived from the branched chain amino acids. You also need TPP in the pentose shunt, which is an important extra-energy and detox pathway. Deficiency of TPP is what eventually shows up as Wernike's encephalopathy and Korsakoff's psychosis among the present day severe alcoholic set.
What is interesting about these old-fashioned deficiency syndromes is that thiamine deficiency today (most commonly seen as Wernike's) isn't the same thing as beriberi. Just as strict vitamin D deficiency isn't quite the same as rickets. With beriberi, there is a clear relationship between the classic symptoms and the amount of carbohydrates in the diet. With Wernike's we know we can bring it on with a bolus of D5W after someone has been living on booze, but Wernike's is missing many of the essential features of beriberi. The modern form is almost entirely confined to the central nervous system.
(It is an assumption nowadays that we have conquered the major deficiency syndromes with science. And, indeed, rickets is rare, beriberi is unknown in the Western world, and anyone ever see a case of pellagra? But my suspicion is that many of our modern diseases are primarily caused by or exacerbated by micronutrient deficiencies. We shouldn't be so complacent. *off soapbox*)
Thiamine, with its key role in central nervous system energy production, can give us clues as to the pathology of syndromes such as Alzheimer's Dementia. Folks with AD have normal thiamine levels, but low levels of the metabolically active TPP, suggesting problems with energy regulation. Giving people with AD extra thiamine can sometimes help the symptoms.
Thiamine, with its key role in central nervous system energy production, can give us clues as to the pathology of syndromes such as Alzheimer's Dementia. Folks with AD have normal thiamine levels, but low levels of the metabolically active TPP, suggesting problems with energy regulation. Giving people with AD extra thiamine can sometimes help the symptoms.
In Japan, there has been a long historical interest in thiamine, and they have come up with a number of synthetic thiamine derivatives. One of them, a disulfide derivative called sulbutiamine, crosses the blood brain barrier more readily than regular thiamine. I don't know much about it, but given the impact of energetics on disorders such as Parkinson's Disease and Alzheimer's, it seems an obvious candidate for further research.
In the mean time, eat your meat, especially if you are a big fan of white rice (though white rice in the US I believe is fortified with thiamine), or alcohol.
In the mean time, eat your meat, especially if you are a big fan of white rice (though white rice in the US I believe is fortified with thiamine), or alcohol.
Thursday, August 25, 2011
Do Carbs Make You Crazy? PCOS and Type II Diabetes Edition
Previously, we discussed the question of Do Carbs Make You Crazy?, reviewed some literature to suggest that a bolus of sugar to a fasting person could certainly make some people crazy (or at least rather rotten-tempered), and yet MIT researchers suggest the same carby bolus will keep people sane with a nice happy squirt of serotonin. Personally I think the MIT advice to snack on marshmallows and pretzels for serenity's sake to be misguided, whereas I agree with the wise orthomolecular doctor from New York who told the young Mr. Ellsberg, suffering from insomnia, grandiosity, and bouts of suicidal depression, to cut out the coffee, alcohol, and sugar already.
(Music - Beastie Boys/Santigold Don't Play No Games That I Can't Win - right click in new tab)
We all agreed, I think, in the comments of the previous posts, that these studies are weakened by some lack of accounting for confounders (nutritional status, alcohol, sleep, insulin resistance, etc. etc. etc. etc.), and of course one can never just change carbohydrates - one has to alter another variable. AND of course I think inflammation and industrial food and micronutrient deficiencies cause or increase insulin resistance and violence and depression… so when one just examines blood glucose level and mood state, one is missing the electrified third rail, so to speak.
And I have to say, the state of the literature ain't that great. Among 15 papers I read for this series, there was one great review paper. Everything else was rather distractingly haphazard. And so we go to two more papers (thanks to Jamie Scott, Jackie, Ambimorph, and Zooko for helping me with the paper chase!): Daily Negative Mood Affects Fasting Glucose in Type 2 Diabetes and The impact of eating behavior on psychological symptoms typical of… (long title - it's about PCOS and blood glucose and mood).
The first paper is about a study following 206 people who kept daily food diaries, morning fasting blood sugar measurements, and daily mood records for 21 days. What is nice about this study is that the participants were phoned every night to get the data for that day. They were also paid $35 for the first week, $45 for the second week, and $55 for the third week, so motivation to keep up with the information gathering was pretty good.
After gathering all the data, there was really only one major finding. There were no real significant correlations between meals, daily mood, and blood glucose - except… if you had a crappy mood one day, you were more likely to have a higher fasting glucose on the morning of the next day. This makes sense if a crappy mood coincides with cortisol increasing, worsening glucose control that is reflected in the next morning's fasting glucose. It doesn't seem to say much about a correlation between carbohydrates and mood in diabetics. There was no relationship between glucose level on day one, for example, and mood on day two.
The second paper with the exhausting title is a little more interesting (well, sort of). This study looked at women with polycystic ovary syndrome (PCOS - known to coincide with insulin resistance), reactive hypoglycemia symptoms, mood, and diet. PCOS affects 10% of women, and between 50-70% of women with PCOS (particularly the lean ones) have symptoms of reactive hypoglycemia. That is, they have a "sugar crash" feeling about 90-120 minutes after a high carb meal. In this study, 24 women with PCOS, 299 controls, 47 self-reported women with symptoms of PCOS, and 92 men filled out an online survey.
Interestingly, 58% of the PCOS group reported having "binge and/or comfort eating" compared with 32% of the control women. More of the PCOS women were also reporting being on a "low-GI diet" - presumably at the advice of their doctors or nutritionists to help control PCOS symptoms. Of the participants, 53% were on no medicines, 13% were on contraception, 5% were on psych meds, 2.2% were on metformin, and 10% were on other meds (typically vitamins or allergy meds). 13% reported psychiatric issues (usually anxiety or depression), and 1.9% reported insulin resistance. The PCOS group was more likely than the controls to have mood or behavioral issues and to have reactive hypoglycemia symptoms.
In a subset of the study, 12 women with PCOS were matched with 12 healthy controls. The women with PCOS were, again, significantly more likely to have reactive hypoglycemia symptoms. Women with PCOS were more likely to have less energy, more tension, less happiness, and more behavioral symptoms associated with hypoglycemia. These differences remained significant after controlling for age, BMI, and "eating behavior."
So what do we find? Women with poor glucose control have, well, poor glucose control, and they have moods and fatigue to match, though underlying inflammation and hormonal badness could cause all of the above. And, not surprisingly, women with poor glucose control have more bingeing and emotional eating - again, perhaps a symptom and a cause wrapped all in one. There were not enough folks on the "low GI" diet to make any intelligible statistical conclusions.
Here's my conclusion. If you have PCOS or type II diabetes, do not eat 300 grams of carbohydrate a day. Don't do it. Keep it low, keep it nutrient rich*, keep it basic happy natural food. I'm guessing your moodiness and your glucose control will improve.
* my idea of nutrient rich and the USDA's idea of nutrient rich are rather different. I think bone marrow and grassfed beef liver are nutrient rich. They prefer skim milk and whole grains. You do the math.
(Music - Beastie Boys/Santigold Don't Play No Games That I Can't Win - right click in new tab)
We all agreed, I think, in the comments of the previous posts, that these studies are weakened by some lack of accounting for confounders (nutritional status, alcohol, sleep, insulin resistance, etc. etc. etc. etc.), and of course one can never just change carbohydrates - one has to alter another variable. AND of course I think inflammation and industrial food and micronutrient deficiencies cause or increase insulin resistance and violence and depression… so when one just examines blood glucose level and mood state, one is missing the electrified third rail, so to speak.
And I have to say, the state of the literature ain't that great. Among 15 papers I read for this series, there was one great review paper. Everything else was rather distractingly haphazard. And so we go to two more papers (thanks to Jamie Scott, Jackie, Ambimorph, and Zooko for helping me with the paper chase!): Daily Negative Mood Affects Fasting Glucose in Type 2 Diabetes and The impact of eating behavior on psychological symptoms typical of… (long title - it's about PCOS and blood glucose and mood).
The first paper is about a study following 206 people who kept daily food diaries, morning fasting blood sugar measurements, and daily mood records for 21 days. What is nice about this study is that the participants were phoned every night to get the data for that day. They were also paid $35 for the first week, $45 for the second week, and $55 for the third week, so motivation to keep up with the information gathering was pretty good.
After gathering all the data, there was really only one major finding. There were no real significant correlations between meals, daily mood, and blood glucose - except… if you had a crappy mood one day, you were more likely to have a higher fasting glucose on the morning of the next day. This makes sense if a crappy mood coincides with cortisol increasing, worsening glucose control that is reflected in the next morning's fasting glucose. It doesn't seem to say much about a correlation between carbohydrates and mood in diabetics. There was no relationship between glucose level on day one, for example, and mood on day two.
The second paper with the exhausting title is a little more interesting (well, sort of). This study looked at women with polycystic ovary syndrome (PCOS - known to coincide with insulin resistance), reactive hypoglycemia symptoms, mood, and diet. PCOS affects 10% of women, and between 50-70% of women with PCOS (particularly the lean ones) have symptoms of reactive hypoglycemia. That is, they have a "sugar crash" feeling about 90-120 minutes after a high carb meal. In this study, 24 women with PCOS, 299 controls, 47 self-reported women with symptoms of PCOS, and 92 men filled out an online survey.
Interestingly, 58% of the PCOS group reported having "binge and/or comfort eating" compared with 32% of the control women. More of the PCOS women were also reporting being on a "low-GI diet" - presumably at the advice of their doctors or nutritionists to help control PCOS symptoms. Of the participants, 53% were on no medicines, 13% were on contraception, 5% were on psych meds, 2.2% were on metformin, and 10% were on other meds (typically vitamins or allergy meds). 13% reported psychiatric issues (usually anxiety or depression), and 1.9% reported insulin resistance. The PCOS group was more likely than the controls to have mood or behavioral issues and to have reactive hypoglycemia symptoms.
In a subset of the study, 12 women with PCOS were matched with 12 healthy controls. The women with PCOS were, again, significantly more likely to have reactive hypoglycemia symptoms. Women with PCOS were more likely to have less energy, more tension, less happiness, and more behavioral symptoms associated with hypoglycemia. These differences remained significant after controlling for age, BMI, and "eating behavior."
So what do we find? Women with poor glucose control have, well, poor glucose control, and they have moods and fatigue to match, though underlying inflammation and hormonal badness could cause all of the above. And, not surprisingly, women with poor glucose control have more bingeing and emotional eating - again, perhaps a symptom and a cause wrapped all in one. There were not enough folks on the "low GI" diet to make any intelligible statistical conclusions.
Here's my conclusion. If you have PCOS or type II diabetes, do not eat 300 grams of carbohydrate a day. Don't do it. Keep it low, keep it nutrient rich*, keep it basic happy natural food. I'm guessing your moodiness and your glucose control will improve.
* my idea of nutrient rich and the USDA's idea of nutrient rich are rather different. I think bone marrow and grassfed beef liver are nutrient rich. They prefer skim milk and whole grains. You do the math.
Sunday, August 21, 2011
Nutritional Brain Bomb - Thiamine Deficiency
Yes, I will get back to the carbohydrate insanity series shortly. But in the comments of the second post, Jack Kruse and Itsthewooo noted that studies with respect to alcohol, blood sugar and violence could be confounded by other nutritional deficiencies. Which is absolutely true. I have to say, it is rare to see scurvy or other famously maritime deficiency diseases aside from the serious long-term alcoholics who frequently populate the emergency room. As one of my attendings in medical school put it, the "Three B diet" (beer, bologna, and bread) is not one likely to come up roses when thrown into a nutritionist's calculator.
So since I seem to be blogging an awful lot right now, I thought I would throw in an instructional primer on brain issues and thiamine deficiency, also known as Wernike's Encephalopathy (and if you are very unlucky, Korsakoff's Psychosis). And a new subset of patients aside from chronic alcoholics need to worry about this issue too - as I mentioned inThe Healthy Skeptic Podcast Chris Kresser Dot Com Podcast Episode 13, there are many case reports in the literature of psychosis and weird psychiatric and neurologic syndromes popping up in gastric bypass patients several years after the surgery - though copper, iron, and B12 are all problematic for post gastric bypass patients, so, apparently, is thiamine (vitamin B1).
Alcohol interferes with the intestinal absorption of thiamine, so that people who obtain the majority of their calories from alcohol are unlikely to get quite enough thiamine. A "clinical pearl" taught in medical school is to double (in your mind, not in the chart!) the amount of alcohol someone tells you he or she drinks. (Hundreds of honest people now vow to halve the amount of drinking they admit to… then realize in truth they already have been…). I've heard every sort of vast quantity of alcohol use daily from "a quart of Jack" or "a 30-pack of beer" to "17 boilermakers" and "whatever I can get my hands on." (Shoot - another "clinical pearl" segue, for any medical students or residents reading this blog - the opposite is actually true for any savvy opiate abusers - often the dose of methadone given to prevent withdrawal is scaled to the amount the patient says he or she uses, rather than using vital signs and clinical picture as is the gold standard, so he or she will often increase the self-reported amount to get more methadone off the bat. And ALWAYS call the methadone clinic to confirm the chronic dose before you write the order for the hospital stay - 160 mg of methadone is a common clinic dose but can stop the breathing of someone not used to that much.)
So who cares if you don't get enough thiamine? Well, as we know, your brain loves energy. As do the rest of your nerves. And good old vitamin B1 is a cofactor to a zillion energetic reactions. If you burn glucose, you desperately need your thiamine. To quote Harrison's Principles of Internal Medicine, 14th Edition (yes, I am old, page 2455):
Yikes! Even if the bigger words are mysterious, let me assure you that the picture is very bad. Dying, rotting neurons and a smokey ruin of your precious brain. Certain areas of the brain, such as the mammilary bodies and parts of the cerebellum seem particularly vulnerable, as they may have some of the highest glucose utilization in the brain. The heart, being a high energy-using fellow itself, is also vulnerable to thiamine deficiency. Nervous system symptoms from thiamine deficiency is also called "dry beriberi" whereas cardiovascular involvement is known as "wet beriberi" or "sailor's asthma."
What are the symptoms? Classically, the clinical triad is paralysis of certain eye movement muscles known as "ophthalmoplegia," problems with balance and walking (often a wide-based, shuffling gait) known as "ataxia," and confusion. Only 1/3 of patients will present with all three - most are very disoriented, inattentive, and sometimes agitated. If a profoundly thiamine-deficient patient shows up in the emergency room and is given straight-up D5 IV drip (D stands for dextrose - which is basically glucose) - this will confound the problem and worsen the symptoms - which can include stupor, coma, and death. (ER docs and nurses really try hard not to kill folks by giving them the standard IV in the emergency room). This is why someone with a history of alcoholism will instead be given a "banana bag" - which contains folate, 100 mg thiamine, magnesium, and a multivitamin solution, which makes the bag yellow instead of clear like most IV solutions (thus the name). Acute thiamine deficiency (Wernike's encephalopathy) can be cured with 50mg thiamine a day until normal eating resumes.
Chronic thiamine deficiency is not curable and can result in a particular type of brain syndrome called Korsakoff's psychosis. The afflicted will have poor memory and confabulate like crazy - meaning, you ask him a question, and he will not know the answer, but he will make one up!
Well, most of you who are not members of the antique navies of the world and also without a 17 boilermaker a day habit or other genetic deficiencies of the pentose phosphate pathway will never experience such severe thiamine deficiency that you will get such dramatic symptoms. But the case of vitamin B1 does serve to illustrate the importance of appropriate nutrition for our noggins to work correctly.
So since I seem to be blogging an awful lot right now, I thought I would throw in an instructional primer on brain issues and thiamine deficiency, also known as Wernike's Encephalopathy (and if you are very unlucky, Korsakoff's Psychosis). And a new subset of patients aside from chronic alcoholics need to worry about this issue too - as I mentioned in
 |
| Wikipedia Commons |
{kind=link}
Alcohol interferes with the intestinal absorption of thiamine, so that people who obtain the majority of their calories from alcohol are unlikely to get quite enough thiamine. A "clinical pearl" taught in medical school is to double (in your mind, not in the chart!) the amount of alcohol someone tells you he or she drinks. (Hundreds of honest people now vow to halve the amount of drinking they admit to… then realize in truth they already have been…). I've heard every sort of vast quantity of alcohol use daily from "a quart of Jack" or "a 30-pack of beer" to "17 boilermakers" and "whatever I can get my hands on." (Shoot - another "clinical pearl" segue, for any medical students or residents reading this blog - the opposite is actually true for any savvy opiate abusers - often the dose of methadone given to prevent withdrawal is scaled to the amount the patient says he or she uses, rather than using vital signs and clinical picture as is the gold standard, so he or she will often increase the self-reported amount to get more methadone off the bat. And ALWAYS call the methadone clinic to confirm the chronic dose before you write the order for the hospital stay - 160 mg of methadone is a common clinic dose but can stop the breathing of someone not used to that much.)
So who cares if you don't get enough thiamine? Well, as we know, your brain loves energy. As do the rest of your nerves. And good old vitamin B1 is a cofactor to a zillion energetic reactions. If you burn glucose, you desperately need your thiamine. To quote Harrison's Principles of Internal Medicine, 14th Edition (yes, I am old, page 2455):
Thiamine is a cofactor of several enzymes, including transketolase, pyruvate dehydrogenase, and alpha-ketoglutarate dehydrogenase. Thiamine deficiency produces a diffuse decrease in cerebral glucose utilization and results in mitochondrial damage… electron microscopy shows disintegrating mitochondria, chromatin clumping, and swelling of degenerating neurons…consistent with excitotoxicity.
Yikes! Even if the bigger words are mysterious, let me assure you that the picture is very bad. Dying, rotting neurons and a smokey ruin of your precious brain. Certain areas of the brain, such as the mammilary bodies and parts of the cerebellum seem particularly vulnerable, as they may have some of the highest glucose utilization in the brain. The heart, being a high energy-using fellow itself, is also vulnerable to thiamine deficiency. Nervous system symptoms from thiamine deficiency is also called "dry beriberi" whereas cardiovascular involvement is known as "wet beriberi" or "sailor's asthma."
What are the symptoms? Classically, the clinical triad is paralysis of certain eye movement muscles known as "ophthalmoplegia," problems with balance and walking (often a wide-based, shuffling gait) known as "ataxia," and confusion. Only 1/3 of patients will present with all three - most are very disoriented, inattentive, and sometimes agitated. If a profoundly thiamine-deficient patient shows up in the emergency room and is given straight-up D5 IV drip (D stands for dextrose - which is basically glucose) - this will confound the problem and worsen the symptoms - which can include stupor, coma, and death. (ER docs and nurses really try hard not to kill folks by giving them the standard IV in the emergency room). This is why someone with a history of alcoholism will instead be given a "banana bag" - which contains folate, 100 mg thiamine, magnesium, and a multivitamin solution, which makes the bag yellow instead of clear like most IV solutions (thus the name). Acute thiamine deficiency (Wernike's encephalopathy) can be cured with 50mg thiamine a day until normal eating resumes.
Chronic thiamine deficiency is not curable and can result in a particular type of brain syndrome called Korsakoff's psychosis. The afflicted will have poor memory and confabulate like crazy - meaning, you ask him a question, and he will not know the answer, but he will make one up!
Well, most of you who are not members of the antique navies of the world and also without a 17 boilermaker a day habit or other genetic deficiencies of the pentose phosphate pathway will never experience such severe thiamine deficiency that you will get such dramatic symptoms. But the case of vitamin B1 does serve to illustrate the importance of appropriate nutrition for our noggins to work correctly.
Saturday, August 20, 2011
Do Carbs Keep You Sane? Midmorning Post-Bagel Slump and the Wurtmans
We are going to rely more on this most excellent review paper by Dr. David Benton of Swansea, UK, Carbohydrate ingestion, blood glucose, and mood to continue our exploration of the question of how ingestion of carbohydrates affects mental state.
First off, some of the short-term studies. We all can guess the results, but a dozen or so studies have shown comparisons between a meal of say, turkey breast versus starch-based meals, or placebo versus a sucrose or glucose containing drink. Not surprisingly, mood/energy measurements at 14-30 minutes after the sugar drinks shows an increase in energy levels, followed by a slump at two hours. In the protein meals versus starchy meals, subjects report a decrease in subjective sense of energy two hours after eating the starchy meal compared to protein. All of these studies were done while subjects were resting quietly.
In studies done of subjects asked to do demanding cognitive tasks (presumably slurping up all available glucose as the noggin is burning nitro), falling levels of reported energy directly correlated with falling blood sugar levels. Subjects with low blood glucose at 30 minutes and 2 hours doing demanding cognitive tests had higher tension ratings than those with high blood glucose. In diabetics, blood glucose levels (measured continuously) have been associated with immediate mood changes, with low corresponding to a more negative mood state than high levels. (There are some interesting perturbations of this phenomena over measurements of days and weeks, however, which I will address in detail in the next post).
Now on to that theory I've actually already discussed at some length in previous posts - via insulin and albumin effects, ingestion of carbohydrate leads to the preferential shuttling of the rare amino acid, tryptophan, into the brain. Since tryptophan is the precursor to serotonin, eating carbohydrates will presumably make one more serene, sleepier, and more sated than someone whose brain is starving for serotonin (low cerebrospinal fluid (CSF) serotonin levels are associated with violence, insomnia, hunger, and suicide, partly because serotonin and its metabolite melatonin play a major role in the mood, appetite, and sleep centers).
Richard and Judith Wurtman of MIT are the ones who originally proposed the theory, and they suggested that humans (particularly premenstrual women and those afflicted with seasonal affective disorder) crave carbs for the serotonin-boosting pharmacologic effect (1)(3). I've seen this theory in textbooks and in research papers many, many times, and I rather took it as fact. Judith Wurtman is a big carb proponent and is likely to give rather strongly-worded quotes to the media damning low-carb diets for causing depression. In the comments, Zooko pointed me to this, er, interesting article by Dr. J. Wurtman for the Huffington Post. Also to her twitter feed, which advises the dubious practice of snacking on pure carbs in between meals for a "serotonin surge" - with specific recommendations for pretzels, rice cakes, and marshmallows. Long term I would say that anyone wanting to lose fat who also has mental health problems should really pretty much avoid adding any processed, micronutrient-poor calories to the mix. What is interesting about the good Dr. Benton's review paper is that he leaves the Wurtmans' tenuous theory crumbled into dust when we look at the context of carbohydrate ingestion in the real world.
It is absolutely true that a carbohydrate only meal after a fast will increase the entry of tryptophan into the brain in rodents, humans, and other primates. The problem is, the moment you eat a bit of food protein, this effect no longer takes place. Dr. Garner was able to increase serotonin in mice brains via a mixed diet, but he fed the little critters extra tryptophan supplements to do the trick (which resulted in increased mouse brain serotonin and a deadly increase in scratching and subsequent skin infections). Without the extra tryptophan boost, as little as 4% of protein in the meal will eliminate the carbohydrate tryptophan-boosting effect. To put that amount of protein into perspective, potatoes, rice, chocolate, and flour all have too much protein for them to increase tryptophan entry into the brain. Bascially, one has to eat pure starch (or a sugary drink) to achieve the pharmacologic carb-serotonin effect, long enough after a previous meal that no protein remains in the gut. That also means that pretzels and rice cakes wouldn't work for a "serotonin surge," and one must stick to marshmallows and jelly beans, which doesn't have much of an evolutionary precedent. This teensy amount of protein killing any "serotonin surge" is true in studies of rats, other primates, and humans (2).
In monkeys, Grimes et al. contrasted protein and carbohydrate breakfasts and found no impact on the levels of cerebrospinal fluid (CSF) tryptophan or serotonin turnover from individual carbohydrate-heavy meals. He went from protein being 25% to 6% of calories, and as protein declined, so did plasma and CSF levels of tryptophan due to lower amounts of raw material protein consumed. There was no immediate change in serotonin turnover or CSF tryptophan levels to individual meals. In the case of the monkeys, higher protein chronically is associated with higher serotonin, not higher carbohydrate, and blood changes of the ratio of tryptophan to other amino acids did not predict CSF tryptophan levels as it does in rats (which are what the Wurtmans studied). I must say the Wurtmans' studies are cited a good deal more often than Benton or Teff or Grimes.
So the carbohydrate = serotonin-increasing theory is likely bogus for humans, especially in the real world (yes, even on Thanksgiving), unless you happen to have a glass of lemonade for breakfast every morning, excluding all other food. BUT, that doesn't mean that carbs don't affect mood. What do studies without such ridiculous attention to actual mechanisms show?
In one study, a drink with 48 grams of carbohydrate and no protein decreased depression, anger, and confusion in women suffering PMS. Judith Wurtman also found that women increased their intake of carbohydrate and fat in the premenstrual stage, and experimental meals with only 4% of the energy as protein did improve the mood of women with PMS. (She did find these women had no higher ratios of tryptophan in their blood than women given control meals, and that women who had improved mood also had no increase in blood levels of tryptophan, suggesting that is not the mechanism for the improved mood) (4).
What do other researchers find? In several reviews, it was found that women generally report an increased craving for sweets and increased appetite in the pre-menstrual period. In humans and animals, there are also changes in basal metabolic rate in the different parts of the cycle, corresponding to the appetite changes, which makes sense. However, a review of studies of what women actually eat showed no difference in the total amount of carbohydrate consumed in any part of the menstrual cycle. Some studies have shown an increase in sweets, chocolate, and cake consumption before and during menses compared to ovulation (which occurs mid-cycle). So there is definite evidence that appetite increases just before and a bit during menstruation, but this corresponds to a higher metabolic rate, and it is foods generally containing a combination of carbohydrate and fat that are craved, not strictly carbohydrates.
In other studies, carbohydrate ingestion has been associated with better mood. De Castro had subjects keep food diaries and mood journals for 9 days, and found that on the days when more carbohydrates were consumed, mood was better (5), and people felt more energetic. He also found a cumulative effect - the more carbohydrate consumed over the week, the happier the person tended to be. In a study of 686 folks who reported their mood at mid-day and what they ate that morning, the more absolute carbohydrate the male subjects consumed that morning, the happier their morning mood. Absolute and relative amounts of protein and fat had no impact on mood in this unpublished study by Benton.
Finally, studies of experimental low carb vs. high carb diets of one week (6), three weeks (7), six weeks (8), and one year (9) show a better comparative mood and increased serenity in the high-carb dieters. The one year study was complicated by the fact that twice as many people in the low-carb group were on antidepressants, and the other studies may have been of too short a duration to bypass the "low carb flu" - and all of those low carb diets may have been high in omega 6. I don't have the energy to chase down all the full texts of all these studies right now (I've seen the year-long one, however), and the one-week one was done in cyclists, who might be cranky in the first week of a low-carb diet while training!
So what have we learned? Well, the Wurtmans and the carbohydrate-tryptophan-serotonin boost theory are scuttled, for now*. But carbohydrates don't seem to cause craziness, and for some people, they seem to help. Is the story any different for folks who have insulin resistance? We'll find out next time (though there might be a quick intervening review of a related topic in between that post and this one).
Please see the later post, Carbs and Serotonin, A Connection After All
First off, some of the short-term studies. We all can guess the results, but a dozen or so studies have shown comparisons between a meal of say, turkey breast versus starch-based meals, or placebo versus a sucrose or glucose containing drink. Not surprisingly, mood/energy measurements at 14-30 minutes after the sugar drinks shows an increase in energy levels, followed by a slump at two hours. In the protein meals versus starchy meals, subjects report a decrease in subjective sense of energy two hours after eating the starchy meal compared to protein. All of these studies were done while subjects were resting quietly.
In studies done of subjects asked to do demanding cognitive tasks (presumably slurping up all available glucose as the noggin is burning nitro), falling levels of reported energy directly correlated with falling blood sugar levels. Subjects with low blood glucose at 30 minutes and 2 hours doing demanding cognitive tests had higher tension ratings than those with high blood glucose. In diabetics, blood glucose levels (measured continuously) have been associated with immediate mood changes, with low corresponding to a more negative mood state than high levels. (There are some interesting perturbations of this phenomena over measurements of days and weeks, however, which I will address in detail in the next post).
Now on to that theory I've actually already discussed at some length in previous posts - via insulin and albumin effects, ingestion of carbohydrate leads to the preferential shuttling of the rare amino acid, tryptophan, into the brain. Since tryptophan is the precursor to serotonin, eating carbohydrates will presumably make one more serene, sleepier, and more sated than someone whose brain is starving for serotonin (low cerebrospinal fluid (CSF) serotonin levels are associated with violence, insomnia, hunger, and suicide, partly because serotonin and its metabolite melatonin play a major role in the mood, appetite, and sleep centers).
Richard and Judith Wurtman of MIT are the ones who originally proposed the theory, and they suggested that humans (particularly premenstrual women and those afflicted with seasonal affective disorder) crave carbs for the serotonin-boosting pharmacologic effect (1)(3). I've seen this theory in textbooks and in research papers many, many times, and I rather took it as fact. Judith Wurtman is a big carb proponent and is likely to give rather strongly-worded quotes to the media damning low-carb diets for causing depression. In the comments, Zooko pointed me to this, er, interesting article by Dr. J. Wurtman for the Huffington Post. Also to her twitter feed, which advises the dubious practice of snacking on pure carbs in between meals for a "serotonin surge" - with specific recommendations for pretzels, rice cakes, and marshmallows. Long term I would say that anyone wanting to lose fat who also has mental health problems should really pretty much avoid adding any processed, micronutrient-poor calories to the mix. What is interesting about the good Dr. Benton's review paper is that he leaves the Wurtmans' tenuous theory crumbled into dust when we look at the context of carbohydrate ingestion in the real world.
It is absolutely true that a carbohydrate only meal after a fast will increase the entry of tryptophan into the brain in rodents, humans, and other primates. The problem is, the moment you eat a bit of food protein, this effect no longer takes place. Dr. Garner was able to increase serotonin in mice brains via a mixed diet, but he fed the little critters extra tryptophan supplements to do the trick (which resulted in increased mouse brain serotonin and a deadly increase in scratching and subsequent skin infections). Without the extra tryptophan boost, as little as 4% of protein in the meal will eliminate the carbohydrate tryptophan-boosting effect. To put that amount of protein into perspective, potatoes, rice, chocolate, and flour all have too much protein for them to increase tryptophan entry into the brain. Bascially, one has to eat pure starch (or a sugary drink) to achieve the pharmacologic carb-serotonin effect, long enough after a previous meal that no protein remains in the gut. That also means that pretzels and rice cakes wouldn't work for a "serotonin surge," and one must stick to marshmallows and jelly beans, which doesn't have much of an evolutionary precedent. This teensy amount of protein killing any "serotonin surge" is true in studies of rats, other primates, and humans (2).
In monkeys, Grimes et al. contrasted protein and carbohydrate breakfasts and found no impact on the levels of cerebrospinal fluid (CSF) tryptophan or serotonin turnover from individual carbohydrate-heavy meals. He went from protein being 25% to 6% of calories, and as protein declined, so did plasma and CSF levels of tryptophan due to lower amounts of raw material protein consumed. There was no immediate change in serotonin turnover or CSF tryptophan levels to individual meals. In the case of the monkeys, higher protein chronically is associated with higher serotonin, not higher carbohydrate, and blood changes of the ratio of tryptophan to other amino acids did not predict CSF tryptophan levels as it does in rats (which are what the Wurtmans studied). I must say the Wurtmans' studies are cited a good deal more often than Benton or Teff or Grimes.
So the carbohydrate = serotonin-increasing theory is likely bogus for humans, especially in the real world (yes, even on Thanksgiving), unless you happen to have a glass of lemonade for breakfast every morning, excluding all other food. BUT, that doesn't mean that carbs don't affect mood. What do studies without such ridiculous attention to actual mechanisms show?
In one study, a drink with 48 grams of carbohydrate and no protein decreased depression, anger, and confusion in women suffering PMS. Judith Wurtman also found that women increased their intake of carbohydrate and fat in the premenstrual stage, and experimental meals with only 4% of the energy as protein did improve the mood of women with PMS. (She did find these women had no higher ratios of tryptophan in their blood than women given control meals, and that women who had improved mood also had no increase in blood levels of tryptophan, suggesting that is not the mechanism for the improved mood) (4).
What do other researchers find? In several reviews, it was found that women generally report an increased craving for sweets and increased appetite in the pre-menstrual period. In humans and animals, there are also changes in basal metabolic rate in the different parts of the cycle, corresponding to the appetite changes, which makes sense. However, a review of studies of what women actually eat showed no difference in the total amount of carbohydrate consumed in any part of the menstrual cycle. Some studies have shown an increase in sweets, chocolate, and cake consumption before and during menses compared to ovulation (which occurs mid-cycle). So there is definite evidence that appetite increases just before and a bit during menstruation, but this corresponds to a higher metabolic rate, and it is foods generally containing a combination of carbohydrate and fat that are craved, not strictly carbohydrates.
In other studies, carbohydrate ingestion has been associated with better mood. De Castro had subjects keep food diaries and mood journals for 9 days, and found that on the days when more carbohydrates were consumed, mood was better (5), and people felt more energetic. He also found a cumulative effect - the more carbohydrate consumed over the week, the happier the person tended to be. In a study of 686 folks who reported their mood at mid-day and what they ate that morning, the more absolute carbohydrate the male subjects consumed that morning, the happier their morning mood. Absolute and relative amounts of protein and fat had no impact on mood in this unpublished study by Benton.
Finally, studies of experimental low carb vs. high carb diets of one week (6), three weeks (7), six weeks (8), and one year (9) show a better comparative mood and increased serenity in the high-carb dieters. The one year study was complicated by the fact that twice as many people in the low-carb group were on antidepressants, and the other studies may have been of too short a duration to bypass the "low carb flu" - and all of those low carb diets may have been high in omega 6. I don't have the energy to chase down all the full texts of all these studies right now (I've seen the year-long one, however), and the one-week one was done in cyclists, who might be cranky in the first week of a low-carb diet while training!
So what have we learned? Well, the Wurtmans and the carbohydrate-tryptophan-serotonin boost theory are scuttled, for now*. But carbohydrates don't seem to cause craziness, and for some people, they seem to help. Is the story any different for folks who have insulin resistance? We'll find out next time (though there might be a quick intervening review of a related topic in between that post and this one).
Please see the later post, Carbs and Serotonin, A Connection After All
Friday, August 19, 2011
Do Carbs Make You Crazy? More About Blood Glucose, Violence, and Mood
I began this series yesterday with a bit of an introduction and some exposure to some differing theories about carbohydrate consumption and mental health (basically they run the gamut from very low carb will spare your mood to you absolutely need carbohydrates for sanity). I didn't take much of a stand, myself, other than to note that in my personal experience, a bit of healthy fat and protein has kept me from experiencing some of the uncomfortable weakness, tremulousness, and crankiness I had a few hours after sugary meals years ago, when, ironically, Stop The Insanity was in vogue.
(Music - Alexander Borodin, Polovtsian Dances, right click to open in new tab)
I noted in my last post that somewhere between 1966 and the early 1990s, it became very unfashionable for medical professionals to endorse the idea of "hypoglycemia," outside of a super low measured blood glucose level of around 40 or less. "Relative (or reactive) hypoglycemia" had been consigned to a psychosomatic diagnosis. So my relative hypoglycemia which predictably occurred at expected physiologic intervals after ingestion of exclusively high-sugar foods or drinks must have been all in my head. :-) In fact, the year before I was born, the American Diabetes Association, the Endocrine Society, and the American Medical Association issued a joint statement on hypoglycemia, stating that widespread publicity "has led the public to believe that there is a widespread and unrecognized occurrence of hypoglycemia in this country… These claims are not supported by the medical evidence." The American Dietetic Association stated: "Valid evidence is lacking to support the hypothesis that reactive hypoglycemia is common cause of violent behavior."
However, when blood glucose falls to quite low levels, the body does tend to react rather aggressively in order to prevent death. Stress hormones, including catecholamines and glucocorticoids, growth hormone, and glucagon are all released. This high-powered combo would no doubt cause sweating, palpitations, anxiety, weakness, crankiness, and other symptoms traditionally associated with hypoglycemia (but can also occur whenever high levels of these hormones are released for any cause) (1 - amazing paper, by the way. I highly recommend it). If the blood glucose falls low enough that the brain is impaired, certainly very bizarre behavior (such as psychosis) can be observed.
How common is such low glucose outside very rare insulin-producing tumors or accidental overdoses of diabetic medications? Well, actually, in oral glucose tolerance tests (the gold standard is when you are given 50 grams of dextrose after an overnight fast, and then blood glucose is measured continuously for up to six hours - often the absolute nadir is missed if the glucose is not measured continuously, but rather at half hour intervals, as is also common), there is a wide range of glucose nadirs in the blood levels of those tested. The average level is about 65, but 10% of people fell below 47, with 2.5% of people below 39. That means that 1 in 40 people could expect to have "true" hypoglycemia in the context of a pure carbohydrate snack after a fast. This effect can be accentuated by caffeine and alcohol.
However, when one goes around measuring glucose levels of typical human beings eating mixed meals (not participating in oral glucose tolerance tests) levels almost never fell below 70. In these healthy subjects, levels pretty much stayed between 70-100 all day long, before and after meals, and overnight. It was a combination of these findings and studies of so-called hypoglycemics whose blood glucose levels did not correlate to symptoms that consigned "relative" or "reactive" hypoglycemia to conservative medical never-never land. However, in my own case, the symptoms were predictable, and the predictable treatment of switching to a higher-protein, higher-fat, less crappy diet cured it, which I would find odd if it were entirely psychosomatic. Also interesting and pointing to a physiologic cause is that the symptoms returned for me during pregnancy - where insulin reactions and "relative" hypoglycemia will tend to be of larger magnitude than in the non-gravid state, in order to promote glucose uptake by the growing fetus.
But there are other very interesting correlates between hypoglycemia and behavior and mood. A researcher named Bolton studied the Peruvian Quolla Indians, who are apparently known as "perhaps the meanest and most unlikeable people on earth." (2) These people, particularly the men, seemed to act out in irrational acts of violence, and also seemed to have very strong sugar cravings. Bolton happened to do glucose tolerance tests in many of the men, and he noticed a statistically significant correlation between the most aggressive subjects and those who had the lowest blood glucose values during the GTT (3). Another researcher, Virkkunen, studied men who had committed serious violent assaults. Their GTTs were also remarkable for higher peak glucose values and subsequently lower glucose nadirs than controls (4). Folks with antisocial personalities have also been noted to have low blood glucose levels, and, once again, it is important to note that many of these men perpetrated the crimes under the influence of alcohol, which will accentuate the hypoglycemic effect. Similar studies in the general population show that both men and women whose blood glucose fall more rapidly during a glucose tolerance test will tend to have higher ratings of aggression (5)(6). In these studies, a glucose level of 63 or lower was strongly associated with the aggressive tendencies. This is still outside a normal healthy humans' blood glucose range eating normal food, but much, much closer to the normal range than 40.
Wow. I guess rapidly fluctuating blood glucose does cause behavioral changes… wait a minute, there, buckaroos - as I had noticed in my perusal of the rather badly reasoned behavior/blood glucose/insulin resistance literature (which I will go over in the next post), and which Inthewooo noted in her comment on the first post in this series, these are mere correlations. Why is the blood glucose changing more rapidly in certain people than others to the same food or glucose stimuli? Could an underlying mechanism explain both aggression and hypoglycemia?
Virkkunen's more violent reactive hypoglycemics had enhanced insulin response to the oral GGT. And it has been found that impulsive offenders who act aggressively, particularly when intoxicated, have lower levels of serotonin turnover (measured low levels of the metabolite of the serotonin metabolite 5-HIAA in the CSF (7)). Low levels of brain serotonin are associated with enhanced insulin secretion and a tendency to develop low blood glucose levels. The data is a bit tenuous, but at least this mechanism makes some sense in the big picture.
Next up - carb craving and chocolate and PMS and Wurtman's rodents! Women with PCOS, reactive hypoglycemia, hyperglycemia, and mood relationships. You might be surprised at what the science shows...
(Music - Alexander Borodin, Polovtsian Dances, right click to open in new tab)
I noted in my last post that somewhere between 1966 and the early 1990s, it became very unfashionable for medical professionals to endorse the idea of "hypoglycemia," outside of a super low measured blood glucose level of around 40 or less. "Relative (or reactive) hypoglycemia" had been consigned to a psychosomatic diagnosis. So my relative hypoglycemia which predictably occurred at expected physiologic intervals after ingestion of exclusively high-sugar foods or drinks must have been all in my head. :-) In fact, the year before I was born, the American Diabetes Association, the Endocrine Society, and the American Medical Association issued a joint statement on hypoglycemia, stating that widespread publicity "has led the public to believe that there is a widespread and unrecognized occurrence of hypoglycemia in this country… These claims are not supported by the medical evidence." The American Dietetic Association stated: "Valid evidence is lacking to support the hypothesis that reactive hypoglycemia is common cause of violent behavior."
However, when blood glucose falls to quite low levels, the body does tend to react rather aggressively in order to prevent death. Stress hormones, including catecholamines and glucocorticoids, growth hormone, and glucagon are all released. This high-powered combo would no doubt cause sweating, palpitations, anxiety, weakness, crankiness, and other symptoms traditionally associated with hypoglycemia (but can also occur whenever high levels of these hormones are released for any cause) (1 - amazing paper, by the way. I highly recommend it). If the blood glucose falls low enough that the brain is impaired, certainly very bizarre behavior (such as psychosis) can be observed.
How common is such low glucose outside very rare insulin-producing tumors or accidental overdoses of diabetic medications? Well, actually, in oral glucose tolerance tests (the gold standard is when you are given 50 grams of dextrose after an overnight fast, and then blood glucose is measured continuously for up to six hours - often the absolute nadir is missed if the glucose is not measured continuously, but rather at half hour intervals, as is also common), there is a wide range of glucose nadirs in the blood levels of those tested. The average level is about 65, but 10% of people fell below 47, with 2.5% of people below 39. That means that 1 in 40 people could expect to have "true" hypoglycemia in the context of a pure carbohydrate snack after a fast. This effect can be accentuated by caffeine and alcohol.
However, when one goes around measuring glucose levels of typical human beings eating mixed meals (not participating in oral glucose tolerance tests) levels almost never fell below 70. In these healthy subjects, levels pretty much stayed between 70-100 all day long, before and after meals, and overnight. It was a combination of these findings and studies of so-called hypoglycemics whose blood glucose levels did not correlate to symptoms that consigned "relative" or "reactive" hypoglycemia to conservative medical never-never land. However, in my own case, the symptoms were predictable, and the predictable treatment of switching to a higher-protein, higher-fat, less crappy diet cured it, which I would find odd if it were entirely psychosomatic. Also interesting and pointing to a physiologic cause is that the symptoms returned for me during pregnancy - where insulin reactions and "relative" hypoglycemia will tend to be of larger magnitude than in the non-gravid state, in order to promote glucose uptake by the growing fetus.
But there are other very interesting correlates between hypoglycemia and behavior and mood. A researcher named Bolton studied the Peruvian Quolla Indians, who are apparently known as "perhaps the meanest and most unlikeable people on earth." (2) These people, particularly the men, seemed to act out in irrational acts of violence, and also seemed to have very strong sugar cravings. Bolton happened to do glucose tolerance tests in many of the men, and he noticed a statistically significant correlation between the most aggressive subjects and those who had the lowest blood glucose values during the GTT (3). Another researcher, Virkkunen, studied men who had committed serious violent assaults. Their GTTs were also remarkable for higher peak glucose values and subsequently lower glucose nadirs than controls (4). Folks with antisocial personalities have also been noted to have low blood glucose levels, and, once again, it is important to note that many of these men perpetrated the crimes under the influence of alcohol, which will accentuate the hypoglycemic effect. Similar studies in the general population show that both men and women whose blood glucose fall more rapidly during a glucose tolerance test will tend to have higher ratings of aggression (5)(6). In these studies, a glucose level of 63 or lower was strongly associated with the aggressive tendencies. This is still outside a normal healthy humans' blood glucose range eating normal food, but much, much closer to the normal range than 40.
Wow. I guess rapidly fluctuating blood glucose does cause behavioral changes… wait a minute, there, buckaroos - as I had noticed in my perusal of the rather badly reasoned behavior/blood glucose/insulin resistance literature (which I will go over in the next post), and which Inthewooo noted in her comment on the first post in this series, these are mere correlations. Why is the blood glucose changing more rapidly in certain people than others to the same food or glucose stimuli? Could an underlying mechanism explain both aggression and hypoglycemia?
Virkkunen's more violent reactive hypoglycemics had enhanced insulin response to the oral GGT. And it has been found that impulsive offenders who act aggressively, particularly when intoxicated, have lower levels of serotonin turnover (measured low levels of the metabolite of the serotonin metabolite 5-HIAA in the CSF (7)). Low levels of brain serotonin are associated with enhanced insulin secretion and a tendency to develop low blood glucose levels. The data is a bit tenuous, but at least this mechanism makes some sense in the big picture.
Next up - carb craving and chocolate and PMS and Wurtman's rodents! Women with PCOS, reactive hypoglycemia, hyperglycemia, and mood relationships. You might be surprised at what the science shows...
Thursday, August 18, 2011
Do Carbs Make You Crazy?
Perhaps I should be more circumspect in my title. After all, there are several popular ideas out there - one that carbohydrates cause blood sugar spikes and crashes, leading to mood swings and general crankiness. The second is that sugar (that special fructosey form of carb) causes everything from ADHD to delinquency to psychosis to bipolar disorder.
(Music selection - Serenade in E Major (right click to open in new tab) by Dvorak, who happened to write what is widely accepted as the most exalted piece of American classical music, though he is in fact fromCzechoslovakia Bohemia.)
I think pretty much everyone has heard of these ideas - most recently I saw them in an article I linked a little while ago, "How I Overcame Bipolar II (and Saved My Own Life)" by Michael Ellsberg. Here is a quote from the article:
Then we have the opposite side of the argument, personified by rodent and women's health researcher Judith Wurtman at MIT, and paleo blogger Don Matesz - carbs improve and are essential for good mood, particularly in the case of PMS, atypical depression, and seasonal affective disorder.
What did I learn in psychiatry residency? Well, that the ideas about sugar causing ADHD were unfounded, and that carbohydrates in general wouldn't be an issue plus or minus unless one had uncontrolled diabetes, in which case, of course, uncontrolled glucose swings could cause all sorts of craziness. Diabetes is one of those conditions we are supposed to rule out before spending 20 hours talking to someone about his or her mother, or prescribing Prozac.
So whom do we believe? Orthomolecular Dr. Hoffman? The Harvard Longwood Psychiatry Residency Training Program? Nora Gedgaudas? Parents who have observed their kids after a party with CAKE and ICE CREAM and FACE-PAINTING FAIRY PRINCESSES? (I'm going to tell you right now that the kids totally spaz out for several hours and then collapse in a twitching exhausted heap of sugar/princess withdrawal. The confounders are many, I must admit).
What have I learned from Gary Taubes and Peter and Kurt? Don't believe anyone. Look it up your own self, and see if it makes sense in the context of physiology and evolution. But y'all know me at this point - let's put aside the issue of metabolic syndrome for a second. Most hunter gatherer societies that I'm aware of ate starch when they could get their hands on it, so it doesn't make sense to me that carbohydrates alone would cause craziness. (We will also leave out alcohol and caffeine which Dr. Hoffman wisely recommends bipolar folks to avoid - both of which will affect SLEEP as well as sugar levels, an obvious confounder in bipolar disorder).
And yet, here on my blog and twitter and elsewhere I've seen reports of folks who feel so much better on VLC diets, and others who feel so much better with zone-ish ratios, and others who do better with more carbohydrates. My own experience (now documented in several podcasts) is that I had hypoglycemia in my late teens and early twenties. Of course, I never got an official diagnosis of hypoglycemia, because that doesn't exist outside the context of diabetes or an insulin overdose or insulin-secreting tumor. If I ate super low fat and high carb, I would get shaky, weak, and cranky about 90 minutes after my last meal. When I called the doctor about it, I was checked for diabetes (negative), and then I was told not to eat like a jerk. (Okay, some days I would eat raspberry fig newtons for lunch and dinner, and I was known to eat an entire package of Peeps from time to time - hey, I was 18.) Eat nuts and avoid sugar, sodas, alcohol, and honey, they told me. Eat snacks. And I was careful from then on out to not be such a jerk about eating and to have snacks - packages of peanuts, apples and string cheese, graham crackers stuffed in my bag - and woe befell anyone in my presence who found me snackless two or three hours after a meal… I don't know how I made it through 7-8 hours of sleep… I personally happen to do better eating a bit more fat, though I'm rarely VLC outside fasting days. I do eat bananas, rice, and potatoes. Yes, it's true.
But what does the literature say? Well, let me begin with a very pleasantly retro article from the halcyon days of 1966, when they believed in hypoglycemia outside of insulin tumors and diabetes - tweeted to me by @ambimorph: Relative Hypoglycemia as a Cause of Neuropsychiatric Illness.
This paper defines "relative hypoglycemia" as my doctor did back in the late 90s - a drop in blood sugar that occurs after eating like a jerk - lots of caffeine or sugar. Apparently the people of the early 20th century suffered from this condition, which was misdiagnosed sometimes as a brain tumor, diabetes, or cerebrovascular problems, but when you stop eating like a jerk and consume some protein, fat, and get rid of the caffeine and alcohol, your symptoms go away.
In 1966 Dr. Salzer found that:
Well. That sounds really bad. It sure does sound like sugar (and caffeine) can make you pretty crazy. And when I (personally) was pregnant, I did suffer from some frank neurologic symptoms related to hypoglycemia (despite the fact that I was eating like Michael Pollan told me to, not like a jerk) - true vertigo, headaches, severe nausea… the thing was, it was all pretty much instantly cured by eating some instant mashed potato flakes. Which is why I know I did not have a brain tumor (not typically responsive to mashed potato therapy). In the modern emergency room we have dextrose IV drips, ginger ale, and instant glucometer measures. I think perhaps that put the end to the mysterious hypoglycemia masking as a brain tumor era of medicine.
Next time… a discussion of carbohydrates and mood, from the literature. And a review of the relationship between blood sugar in mood in folks with diabetes, insulin resistance, and women with PCOS.
(Music selection - Serenade in E Major (right click to open in new tab) by Dvorak, who happened to write what is widely accepted as the most exalted piece of American classical music, though he is in fact from
I think pretty much everyone has heard of these ideas - most recently I saw them in an article I linked a little while ago, "How I Overcame Bipolar II (and Saved My Own Life)" by Michael Ellsberg. Here is a quote from the article:
Dr. Hoffman told me there is mounting clinical evidence linking mood swings to blood sugar issues, and that in his experience bipolar patients respond well to cutting out refined sugar, and coffee and alcohol (which affect blood sugar) from their diets. “You should stop eating refined sugar altogether, and stop drinking alcohol and coffee,” he told me.Apparently, Mr. Ellsberg went to a psychiatrist also:
I asked the psychiatrist I was seeing at the time whether he thought there was any link between nutrition and mental health. He looked at me as though I had just asked whether there was any link between mental health and UFO rectal probes. “There is absolutely no evidence of any link whatsoever between dietary choices and mental health,” he said curtly, and changed the subject.Besides my wacky UFO rectal probe blog, on the paleo mental health side of things we have Nora Gedgaudas, who has just released an updated version of Primal Body, Primal Mind. I have read her book, and though I did not attend her talk at AHS, from my memory of her book and the coverage of that talk, it seems to me she advocates a very low carbohydrate approach, that in effect we are either fat burners or sugar burners, and fat burners are steady and serene, while sugar burners are moody and cranky. (Nora herself! clarifies her very reasonable position in the comments below - in short, her clinical experience has shown her that limiting sugars and starches for most people has been very helpful.)
Then we have the opposite side of the argument, personified by rodent and women's health researcher Judith Wurtman at MIT, and paleo blogger Don Matesz - carbs improve and are essential for good mood, particularly in the case of PMS, atypical depression, and seasonal affective disorder.
What did I learn in psychiatry residency? Well, that the ideas about sugar causing ADHD were unfounded, and that carbohydrates in general wouldn't be an issue plus or minus unless one had uncontrolled diabetes, in which case, of course, uncontrolled glucose swings could cause all sorts of craziness. Diabetes is one of those conditions we are supposed to rule out before spending 20 hours talking to someone about his or her mother, or prescribing Prozac.
So whom do we believe? Orthomolecular Dr. Hoffman? The Harvard Longwood Psychiatry Residency Training Program? Nora Gedgaudas? Parents who have observed their kids after a party with CAKE and ICE CREAM and FACE-PAINTING FAIRY PRINCESSES? (I'm going to tell you right now that the kids totally spaz out for several hours and then collapse in a twitching exhausted heap of sugar/princess withdrawal. The confounders are many, I must admit).
What have I learned from Gary Taubes and Peter and Kurt? Don't believe anyone. Look it up your own self, and see if it makes sense in the context of physiology and evolution. But y'all know me at this point - let's put aside the issue of metabolic syndrome for a second. Most hunter gatherer societies that I'm aware of ate starch when they could get their hands on it, so it doesn't make sense to me that carbohydrates alone would cause craziness. (We will also leave out alcohol and caffeine which Dr. Hoffman wisely recommends bipolar folks to avoid - both of which will affect SLEEP as well as sugar levels, an obvious confounder in bipolar disorder).
And yet, here on my blog and twitter and elsewhere I've seen reports of folks who feel so much better on VLC diets, and others who feel so much better with zone-ish ratios, and others who do better with more carbohydrates. My own experience (now documented in several podcasts) is that I had hypoglycemia in my late teens and early twenties. Of course, I never got an official diagnosis of hypoglycemia, because that doesn't exist outside the context of diabetes or an insulin overdose or insulin-secreting tumor. If I ate super low fat and high carb, I would get shaky, weak, and cranky about 90 minutes after my last meal. When I called the doctor about it, I was checked for diabetes (negative), and then I was told not to eat like a jerk. (Okay, some days I would eat raspberry fig newtons for lunch and dinner, and I was known to eat an entire package of Peeps from time to time - hey, I was 18.) Eat nuts and avoid sugar, sodas, alcohol, and honey, they told me. Eat snacks. And I was careful from then on out to not be such a jerk about eating and to have snacks - packages of peanuts, apples and string cheese, graham crackers stuffed in my bag - and woe befell anyone in my presence who found me snackless two or three hours after a meal… I don't know how I made it through 7-8 hours of sleep… I personally happen to do better eating a bit more fat, though I'm rarely VLC outside fasting days. I do eat bananas, rice, and potatoes. Yes, it's true.
But what does the literature say? Well, let me begin with a very pleasantly retro article from the halcyon days of 1966, when they believed in hypoglycemia outside of insulin tumors and diabetes - tweeted to me by @ambimorph: Relative Hypoglycemia as a Cause of Neuropsychiatric Illness.
This paper defines "relative hypoglycemia" as my doctor did back in the late 90s - a drop in blood sugar that occurs after eating like a jerk - lots of caffeine or sugar. Apparently the people of the early 20th century suffered from this condition, which was misdiagnosed sometimes as a brain tumor, diabetes, or cerebrovascular problems, but when you stop eating like a jerk and consume some protein, fat, and get rid of the caffeine and alcohol, your symptoms go away.
In 1966 Dr. Salzer found that:
…patients with relative hypoglycemia have been diagnosed as having psychoneurotic anxiety, psychoneurotic depression, depressive reactions, schizophrenia, manic-depressive psychosis, psychopathic personality, chronic alcoholism, convulsive disorders, migraine, idiopathic cephalalgia, second cervical root syndrome, neurodermatitis, and even hypertensive cardiovascular disease... Major symptoms from a psychiatric standpoint are depression, insomnia, anxiety, irritability, lack of concentration, crying spells, phobias, forgetfulness, confusion… antisocial behavior, and suicidal tendencies… The major neurological symptoms are headache, dizziness, inward and external tremulousness, numbness, blurred vision, staggering, fainting or blackouts, and muscular twitching...There are also extensive somatic symptoms as follows: exhaustion, fatigue, sweating, anorexia, tachycardia, cold hands and feet, obesity, chronic indigestion, bloating, abdomnial spasm, muscle and joint pains, backache, muscle cramps, colitis, and convulsions.
Well. That sounds really bad. It sure does sound like sugar (and caffeine) can make you pretty crazy. And when I (personally) was pregnant, I did suffer from some frank neurologic symptoms related to hypoglycemia (despite the fact that I was eating like Michael Pollan told me to, not like a jerk) - true vertigo, headaches, severe nausea… the thing was, it was all pretty much instantly cured by eating some instant mashed potato flakes. Which is why I know I did not have a brain tumor (not typically responsive to mashed potato therapy). In the modern emergency room we have dextrose IV drips, ginger ale, and instant glucometer measures. I think perhaps that put the end to the mysterious hypoglycemia masking as a brain tumor era of medicine.
Next time… a discussion of carbohydrates and mood, from the literature. And a review of the relationship between blood sugar in mood in folks with diabetes, insulin resistance, and women with PCOS.
Tuesday, August 16, 2011
AHS 2011 Presentation - Slides and Video
Just in case you missed them:
Next up, I will look at carbohydrates, blood glucose, and mood connections.
Saturday, August 13, 2011
Neuroregulation of Appetite
The cause of obesity has been a hot topic in the paleoblogosphere lately. Let me be the first to tell you that I am no obesity researcher or expert (there, first point goes to Itsthewooo). All I know is that a few percentage of folks have been obese for thousands of years. And back in the late 1870s, here's a picture of my great great great (etc.) grandfather's funeral - you might have to click on it to enlarge and squint a bit, but I really don't see any obese people there.






Fast forward to 1919 - here's my grandmother, her mother, and her mother. Babies were chubby-cheeked as was my great great grandmother. They lived in the same area and were of the same socioeconomic class as many of the people in the first photograph.

And now 1943. My father is the baby in this next picture. As you can see, the children and young or middle-aged adults (including the middle-aged women who have had children) are lean, whereas the older folks have some extra adipose, especially around the middle (again, same area of the country):

And then 1987 - this picture is a tour of the USS Constitution in Charlestown, MA. As you can see, middle aged folks and even the kids are starting to be chubby, especially around the middle:

These pictures don't tell us much about what we don't already know. Obesity is a 20th and 21st century disease, that came upon us younger and younger as the decades rolled along, accelerating since 1980 or so.
What caused it? Video games? Captain Crunch commercials? Environmental toxins? I don't know, but my money is still on the food. Somewhere between the diets of the Kitavans and the Sioux and most of the people in the world before 1900 and our current diets is the cause of obesity.
Dr. Pendergrass of the University of Kansas had a great poster presentation up at AHS about the neuroregulation of appetite. He painstakingly cobbled together a fantastic diagram that detailed the communications between different organ systems, adipose tissue, and the brain. He highly recommended this paper if you are interested: Stress, eating, and the reward system.
Dr. Pendergrass' diagram was highly technical, inclusive, and awesome, though he warned me that he left out "about 120 known hormonal signals" between the GI tract and the brain. His also had a great deal of detail regarding the brain and different areas of it, along with specific hormonal and molecular signals and feedback there. Here is my layperson's version, which leaves out all the crushing detail. I can't promise all the arrows are leading the right direction (a graphic designer I am not):

It's complicated. Yeah, leptin, insulin, amylin, CCK, glucose, fat, etc. are all involved. Yes, once you have metabolic syndrome, dropping the carbohydrate will likely help (how low for how long? Beats me.) If you have advanced types of certain kinds of neurologic disease, there's evidence a ketogenic diet can be helpful. Make sure your micronutrient status is tip top and eliminate food toxins. Real, evolutionary medicine-inspired food is the easiest way to do that sort of thing.
But anyone who says he or she completely understands obesity is probably lying.
Friday, August 12, 2011
Omega 3, Inflammation, and Anxiety in Medical Students
During all the fist-pumping, bright, sparkly eye-admiring, and general back-slapping of the inaugural Ancestral Health Symposium last weekend, the world of academia rolled on, and some cool evolutionary psychiatry-type papers were published. Today's entry reviews a neat paper from my favorite journal, Brain, Behavior, and Immunity. Omega-3 supplementation lowers inflammation and anxiety in medical students: a randomized controlled trial. Somehow I missed it in all the pre-conference hoopla, but as usual Jamie was Johnny-on-the-spot and emailed me the link. And he thinks I'm the nerd. :-)
This paper combines a lot of positives - a randomized controlled trial, using actual blood metrics (plasma 6:3 ratios and PBMC 6:3 ratios along with measurements of inflammatory cytokines.) And they weren't completely stupid with the placebo (so many RCTs of omega 3 supplementation in mental health use soybean oil or olive oil placebos - both of which can throw a huge question mark into the results, as both may have their own mental health effects).
Let's begin with the interesting stuff from the introduction. Inflammation is related to all sorts of bad mojo like heart disease, autoimmune disease, stroke, and mental illness. Populations that eat more fish tend to suffer less from these diseases, and it is felt that the omega-3 PUFAs in fish may be protective against inflammation. Epidemiological data and observational studies have shown higher fish or DHA and EPA intake is associated with lower incidence of depressive disorders, both in non-psychiatrically ill and psychiatrically ill populations. The randomized controlled trials of omega 3 supplementation have had mixed results, with an overall trend for improving clinical depression, but not necessarily sub-clinical depressed mood. The data for anxiety disorders is less robust - lower omega-3 plasma levels are found in folks with social anxiety, but two small RCTs of supplementation in anxiety also had mixed results. It is important to know that both anxiety and depression are associated with an increase in pro-inflammatory cytokines - most commonly measured ones are IL-6 and TNFalpha.
Very roughly (for more info, visit Anastasia's latest post), omega 3 fatty acids become anti-inflammatory cytokines, and omega 6 fatty acids become inflammatory cytokines (as always in biochemistry that is not the whole story, but it will work for our purposes today). Therefore, increasing omega 3s will help reduce inflammation, or so goes the theory. My favorite grumpy Belgian Dr. Maes had a cool paper out in 2000 showing that medical students with worse (ie higher) serum 6:3 ratios had higher increases in inflammatory markers (LPS and TNFalpha) during exam times. Interesting. Let's see what happens in the medical students from today's paper.
Over the course of a few years, several cohorts of a total of 68 medical students, aged 21-29, 38 men and 30 women, were randomized to either an omega 3 supplement of 2085mg EPA and 348 mg DHA (I think this is the OmegaBrite supplement sold by a Harvard psychiatrist, Andy Stoll - I think he led a grand rounds for us, but I don't know him personally) or placebo. The placebo was a mixture of palm, olive, soybean, canola, and coco butter oils meant to mimic standard fatty acid ratios consumed by adults in the US. The placebo also had a fish flavoring added to keep the experiment blinded. The supplementation went on for about 12 weeks total, and data was collected before, during (critically, the day before major exams) and several months after supplementation was discontinued.
The fatty acid ratios were studied in an interesting way - first straight-up plasma levels were measured, then levels were measured from inflammation-stimulated cultures of peripheral blood mononuclear cells (PBMCs, like lymphocytes). Que? Well, the reservoir of active omega 6 and omega 3 precursors to our inflammatory or anti-inflammatory response is housed on our cell membranes - so when you stimulate these immune T or B cells with an inflammatory signal (typically LPS is used), they start spitting out cytokines in response, the level of inflammatory response depending upon what raw omega 3 or omega 6 materials they have. So in this experiment, not only was the straight-up omega 6 to omega 3 ratio in the blood measured, so was the simulated omega 6 and omega 3 inflammatory/anti-inflammatory immune response itself. Kinda neat. All right.
Results! An impressive 67 of the 68 students completed the trial (med students are dutiful). Any "habitual fish-eaters" and anyone on omega-3 supplementation or other inflammation-modulating medication or supplement regimen was excluded, along with anyone with any health problems or any smokers. At the beginning, levels of the omega 3s DHA and EPA were about the same across all groups - by the third blood draw, plasma levels of EPA and DHA were 6-fold and 1/2-fold higher in the experimental group than in controls. The levels in the PMBCs were 3 fold and 1/3 fold higher than in controls.
As for the inflammatory response and anxiety levels in the students, supplementation reduced the levels of IL-6 and TNFalpha by 14% in the experimental group, and anxiety scores (which were low across all groups at all measured times) were also decreased by 20% in the experimental group. There was no change in the amount of inflammation at exam-time, unlike in the previous Maes study.
The researchers found these results to be pretty exciting - especially as this was a young, healthy population. The average 6:3 ratio at baseline was 10.82, which is quite a bit lower than the population averages of 15-17:1 (though markedly higher than Cordain's estimates of 3:1 in hunter-gatherers). Baseline levels of IL-6 and TNFalpha for all the medical students were lower than the population average and baseline intake of EPA+DHA in these students was 70% higher than their national age peers. So even though these medical students had better ratios and less simmering inflammation than the general population and were perhaps a poor choice for this particular study, the OmegaBrite intervention significantly decreased the inflammatory response, and the changes might have been more marked in a more typical American population. And, indeed, previous randomized controlled trials of omega 3 PUFA supplementation have rather consistently produced decreased inflammation in the elderly, diabetics, and folks with high triglycerides.
This study is the first one to show anxiolytic effects of omega 3 supplementation in a population without baseline anxiety. Depression scores (like the anxiety scores, low at baseline) were not affected - which is in concordance with the large body of evidence showing omega-3 PUFA supplementation can be effective for clinical but not sub-clinical depression.
The paper ends with an interesting discussion of the safety of omega-3 fatty acid supplementation - at these low amounts, there is not an increase in hemorrhagic stroke or bleeding time, even in combination with aspirin. Epidemiologic studies show decreased risk of dying from pneumonia, reduction in post-surgical infections, and much lower risk of thrombotic stroke in folks who eat more fish. The FDA deems that doses up to 3 grams per day of marine PUFAs are "generally recognized as safe."
So - medical students - 2.5g daily of EPA/DHA equals 20% less anxiety and 14% less inflammation. Everyone else might benefit even more. Since we know by taste that fish aren't rotten (I hope), I think it is safest to get fish oil from fish (wild-caught and sourced carefully to avoid PCBs and heavy metals), and safer still to limit all easily oxidized PUFAs (6 and 3) in the diet to the minimal requirements we need.
* My big omega 3 post can be found here: Your Brain on Omega 3
* Biochem nerds will want to check out this paper by Omega 3 Heavy Hitter Artemis Simopoulos
This paper combines a lot of positives - a randomized controlled trial, using actual blood metrics (plasma 6:3 ratios and PBMC 6:3 ratios along with measurements of inflammatory cytokines.) And they weren't completely stupid with the placebo (so many RCTs of omega 3 supplementation in mental health use soybean oil or olive oil placebos - both of which can throw a huge question mark into the results, as both may have their own mental health effects).
Let's begin with the interesting stuff from the introduction. Inflammation is related to all sorts of bad mojo like heart disease, autoimmune disease, stroke, and mental illness. Populations that eat more fish tend to suffer less from these diseases, and it is felt that the omega-3 PUFAs in fish may be protective against inflammation. Epidemiological data and observational studies have shown higher fish or DHA and EPA intake is associated with lower incidence of depressive disorders, both in non-psychiatrically ill and psychiatrically ill populations. The randomized controlled trials of omega 3 supplementation have had mixed results, with an overall trend for improving clinical depression, but not necessarily sub-clinical depressed mood. The data for anxiety disorders is less robust - lower omega-3 plasma levels are found in folks with social anxiety, but two small RCTs of supplementation in anxiety also had mixed results. It is important to know that both anxiety and depression are associated with an increase in pro-inflammatory cytokines - most commonly measured ones are IL-6 and TNFalpha.
Very roughly (for more info, visit Anastasia's latest post), omega 3 fatty acids become anti-inflammatory cytokines, and omega 6 fatty acids become inflammatory cytokines (as always in biochemistry that is not the whole story, but it will work for our purposes today). Therefore, increasing omega 3s will help reduce inflammation, or so goes the theory. My favorite grumpy Belgian Dr. Maes had a cool paper out in 2000 showing that medical students with worse (ie higher) serum 6:3 ratios had higher increases in inflammatory markers (LPS and TNFalpha) during exam times. Interesting. Let's see what happens in the medical students from today's paper.
Over the course of a few years, several cohorts of a total of 68 medical students, aged 21-29, 38 men and 30 women, were randomized to either an omega 3 supplement of 2085mg EPA and 348 mg DHA (I think this is the OmegaBrite supplement sold by a Harvard psychiatrist, Andy Stoll - I think he led a grand rounds for us, but I don't know him personally) or placebo. The placebo was a mixture of palm, olive, soybean, canola, and coco butter oils meant to mimic standard fatty acid ratios consumed by adults in the US. The placebo also had a fish flavoring added to keep the experiment blinded. The supplementation went on for about 12 weeks total, and data was collected before, during (critically, the day before major exams) and several months after supplementation was discontinued.
The fatty acid ratios were studied in an interesting way - first straight-up plasma levels were measured, then levels were measured from inflammation-stimulated cultures of peripheral blood mononuclear cells (PBMCs, like lymphocytes). Que? Well, the reservoir of active omega 6 and omega 3 precursors to our inflammatory or anti-inflammatory response is housed on our cell membranes - so when you stimulate these immune T or B cells with an inflammatory signal (typically LPS is used), they start spitting out cytokines in response, the level of inflammatory response depending upon what raw omega 3 or omega 6 materials they have. So in this experiment, not only was the straight-up omega 6 to omega 3 ratio in the blood measured, so was the simulated omega 6 and omega 3 inflammatory/anti-inflammatory immune response itself. Kinda neat. All right.
Results! An impressive 67 of the 68 students completed the trial (med students are dutiful). Any "habitual fish-eaters" and anyone on omega-3 supplementation or other inflammation-modulating medication or supplement regimen was excluded, along with anyone with any health problems or any smokers. At the beginning, levels of the omega 3s DHA and EPA were about the same across all groups - by the third blood draw, plasma levels of EPA and DHA were 6-fold and 1/2-fold higher in the experimental group than in controls. The levels in the PMBCs were 3 fold and 1/3 fold higher than in controls.
As for the inflammatory response and anxiety levels in the students, supplementation reduced the levels of IL-6 and TNFalpha by 14% in the experimental group, and anxiety scores (which were low across all groups at all measured times) were also decreased by 20% in the experimental group. There was no change in the amount of inflammation at exam-time, unlike in the previous Maes study.
The researchers found these results to be pretty exciting - especially as this was a young, healthy population. The average 6:3 ratio at baseline was 10.82, which is quite a bit lower than the population averages of 15-17:1 (though markedly higher than Cordain's estimates of 3:1 in hunter-gatherers). Baseline levels of IL-6 and TNFalpha for all the medical students were lower than the population average and baseline intake of EPA+DHA in these students was 70% higher than their national age peers. So even though these medical students had better ratios and less simmering inflammation than the general population and were perhaps a poor choice for this particular study, the OmegaBrite intervention significantly decreased the inflammatory response, and the changes might have been more marked in a more typical American population. And, indeed, previous randomized controlled trials of omega 3 PUFA supplementation have rather consistently produced decreased inflammation in the elderly, diabetics, and folks with high triglycerides.
This study is the first one to show anxiolytic effects of omega 3 supplementation in a population without baseline anxiety. Depression scores (like the anxiety scores, low at baseline) were not affected - which is in concordance with the large body of evidence showing omega-3 PUFA supplementation can be effective for clinical but not sub-clinical depression.
The paper ends with an interesting discussion of the safety of omega-3 fatty acid supplementation - at these low amounts, there is not an increase in hemorrhagic stroke or bleeding time, even in combination with aspirin. Epidemiologic studies show decreased risk of dying from pneumonia, reduction in post-surgical infections, and much lower risk of thrombotic stroke in folks who eat more fish. The FDA deems that doses up to 3 grams per day of marine PUFAs are "generally recognized as safe."
So - medical students - 2.5g daily of EPA/DHA equals 20% less anxiety and 14% less inflammation. Everyone else might benefit even more. Since we know by taste that fish aren't rotten (I hope), I think it is safest to get fish oil from fish (wild-caught and sourced carefully to avoid PCBs and heavy metals), and safer still to limit all easily oxidized PUFAs (6 and 3) in the diet to the minimal requirements we need.
* My big omega 3 post can be found here: Your Brain on Omega 3
* Biochem nerds will want to check out this paper by Omega 3 Heavy Hitter Artemis Simopoulos
Thursday, August 11, 2011
AHS 2011 - MovNat at Venice Beach
One of the benefits of being an AHS presenter was an opportunity to attend a MovNat One-day Workshop on Venice Beach the day after AHS. I'm actually surprised that more presenters did not take advantage of the opportunity - however, I know that Melissa McEwen and Richard Nikoley had done the 5-day workshops in West Virginia (and Robb Wolf, Metzgar, and John Durant also have MovNat experience, according to Erwan), while some of the other presenters don't look quite like the tree-climbing type. But among some AHS attendees, volunteers, and (shockingly) people from southern California who had no idea about AHS were Dr. BG, her sister, Dr. Eenfeldt, Jamie Scott, and myself. On that foggy Sunday morning we arrived in vibrams, barefoot, or in other barefootesque shoes to the bleachers next to "muscle beach" at 8:45am sharp.



 |
| Clifton Harski and Attendees at Muscle Beach |
Why MovNat? Well, of course, the best advertisement for this particular fitness method is its teachers - in America, Clifton Harski (in images ruthlessly swiped from his blog):

And, of course, the legendary French founder of MovNat, Erwan le Corre, also known as the World's Fittest Man, who had a great talk on the second day of AHS proper.

Let's just say that when the shirts came off as the weather warmed up, the whistles from Venice Beach were not for me. (In full disclosure, I did not remove my shirt).
 |
| Erwan giving initial instructions |
MovNat is actually very simple (in some ways deceivingly so). We learned to run, carry, lift, climb, throw, crawl, and balance, and more importantly to think about moving in a natural human way. Most of us had spent many hours in the gym learning to isolate body parts and perform exercises to maximize both muscle burn and safety - but often these stereotyped movements have little utility (other than basic strength or stamina) when it comes to survival on planet Earth. Sure, you can do a pull-up on a bar - can you do a pull up on a wider tree branch? Or a step? Can you lift a rock instead of a barbell? Maybe you have a 6 minute mile on a track, but how fast and efficiently can you move on the trail, through the jungle, requiring ducking, crawling, careful foot placement, balance, and jumping past obstacles. When you sit up, do you muscle yourself up like at the gym, or do you raise your legs and flop up efficiently as you did when you were a kid? Guess which one is the MovNat way?
Jungle running, climbing, and balancing sound intimidating. And even though I go to Crossfit, I'm pretty much the weakest one at the gym, and I've always been more likely to be picked last for a sports team than first. I wanted to go to MovNat because I don't think that I move all that well. What surprised me is that I was already good at many things we were asked to do. People at the workshop were every fitness level - from RKC kettlebell instructor/gym owners to parkour enthusiasts to chiropractors, a family medicine doctor from my hometown, a radiologist, and a mom who walks on the beach, yet everyone seemed to learn something, and each exercise was scaled for all fitness levels.
I cannot, typically, do a standard pull-up from a dead hang. I just don't have the upper body strength (yet). Sometimes I'm able to crank one out - if I'm not tired and I cheat a little - and I can do a chin-up, but I was able to climb on top of the bars at Venice Beach multiple times using the most efficient strategy taught by Erwan. (I did end up with some pretty intense bruises from the climbing - but that's just because I was so exhilarated getting on top of that bar!) I could also climb a pole and fireman carry some surprisingly heavy fellow paleo bloggers.
There was considerable time in the day for rest, recovery, and reflection. In those times Erwan and Clifton explained some of the MovNat philosophy. As a psychiatrist, I see plenty of Zoo Humans like myself, most very much afflicted by the painful incongruence between or modern world and the natural world to which we are evolved. This difference plagues our minds as well as our bodies. Erwan plugged some relaxation and mindful living very much in line with what the academics who study mindfulness will teach - live in the moment, exist using your senses, cultivate thinking using the "third eye" or the eye at the top of the pyramid (like on the dollar bill) above yourself, not within yourself (Erwan did not use that exact analogy but something very similar), and don't think so much in general. Sleep late if you need to! (I'm thinking Erwan does not have small children). Swing from trees. Be happy and gorgeous and human.
The day was not without struggle and suffering - also a large part of being human.
For me, I hope to encourage my kids to climb trees and balance and play tag and move - while they teach me the other secrets of natural, efficient human movement they do all on their own. I'm also seriously considering a 7-day workshop in Thailand (one of my work colleagues would love to go too). A week without shoes, suffering in the jungle sounds just about perfect.
Just one more note about the instructors - I could not describe Erwan as down-to-earth (perhaps because I keep imagining his home in Santa Fe as a tree house*), but he was funny, generous, and an exceptional person. He heals bodies and minds and bridges the natural world with the flamboyant setting of Venice Beach with a somewhat unearthly serenity (ironically, his serenity is most likely derived from the natural world - so perhaps very earthly). Clifton was his perfect foil - practical, organized, also funny, and very approachable. He has a degree in kinesiology and sought out MovNat because he saw the incomplete picture of all the zillion different fitness methods in which he had immersed himself.
So, all in all, if you have basic mobility and can hang from a bar, you will learn something from MovNat. It's innate, deceivingly simple, and marvelous.
* (I have no idea what Erwan le Corre's home looks like)
 |
| Look what Erwan and Clifton made me do today (Saturday August 13th, 2011)! |
Tuesday, August 9, 2011
AHS - The People Post
I was excited to see the talks at the Ancestral Health Symposium, but let's face it, I've been to enough talks in my career to make me want to dismantle powerpoint template by template and declare victory. The real reason I wanted to go to AHS was to meet the people. The funky, fit, fabulous, barefooted paleo people. It can be lonely being the only grain-eschewing fat-eating mom at the preschool open house, and even lonelier being an evolutionary medicine inspired doctor. So to hang out with a bunch of like-minded souls in person - well, that was fun.
I was very gratified and surprised to find two evolutionary medicine psychiatrists who had come to the conference and went out of their way to speak to me. We talked some shop and how to safely integrate evolutionary medicine principles - and how to document it, which in a medicolegal sense is absolutely key. They had some terrific ideas, and it was encouraging.
But the psychiatrists and the other people, the ones you know from the internets, they were amazing. Stephan Guyenet and Clifton Harski both noted in their most recent blog posts that overall it was a fit, attractive, and healthy-looking group. Obviously radical ancestral health enthusiasts will be self-selecting for health conscious people - but it was a stunning advertisement for the lifestyle. There was also, in general, a high level of positivism and intelligence.
Now some pictures - from my iphone 3GS, so don't expect too much.
I have to run now, but will come back tonight and edit with more reflections on (more) people and experiences….
… I'm back. All right! Now the dirt! Just kidding. I just wanted to mention my impressions of the many I met - and if I skip you, I'm terribly sorry.
Jamie Scott - Awesome, humble fellow who came all the way out from New Zealand to help liven up my presentation and to meet and connect with the other AHS folks. I knew up front with the presentation we were going to have to hang out a bit, which can be a risk with someone you have never met. However, we were buddies from the get-go, and it was terrific to present with him and to show him around Los Angeles a little, as it was his first visit to the States. Jamie is a skeptic, as I am, and an excellent person to discuss ideas with. He also (fortunately) never seems to tire of talking paleo!
Folks from the presenter/volunteer party: Dr. BG - amazing, vibrant and gorgeous as we knew already. Down to earth and practical, which I actually wouldn't expect from her blogging, which is aways a cross between rock and roll, hotness, and amazing anthropology and pharmacology. Her sister was also very nice and gave me her extra chcocolate bar after my presentation. They both came to MovNat, and that was an amazing experience. Denise Minger - I had a chance to chat with her later on Saturday night, but I just have to echo everyone else's sentiments about her being bubbly and delightful. Richard and Bea Nikoley - who looked great, tanned, and were among the first (of many) to remark about how young I am. Let the record now show that I am 37. So younger than some, and older than many!
The Drs. Eades - formidable presence, lovely to talk to. I do admire their ability to practice the medicine they felt was right in the low-fat heyday of the 80s and 90s. Were I an obesity doctor back then, I would have lost my mind and wandered off into the wilderness. Bryan Barksdale - this young man is starting life as an MD/PhD student. Funnily enough, we both went to the same high school. Aaron Blaisdell and Brent Pottenger - I can only imagine the amount of work that went into organizing the symposium. Thank you, thank you, thank you. Andrew "Evolvify" - I still haven't got you figured out; I respect the genius and mostly just sit back and absorb the blog. He reminded me of some of my friends from back home in Austin, who tend to be brilliant and a bit off the beaten path. Stephan Guyenet - I hate to use the term "adorable" for him, but it describes him completely, from his relaxing zen personality to his amazing brain. I owe Stephan a lot as his blog helped me get a holistic head or tails of the evolutionary medicine piece - and his blog drives a lot of traffic to mine ;-)
Melissa McEwen and Chris Masterjohn I had met before, and I greatly admire their persistence in chasing down truth, and excellence in analysis of papers. John Durant and I had a discussion about writing books - his sounds well on its way. He's very down-to-earth and approachable. Clifton Harski and Erwan Le Corre - I will talk more about them in my MovNat post. Dr. Pendergrass had called me before to discuss the neuroregulation of obesity, he is not a blogger, but teaches biochemistry to med students, and is intense and enthusiastic about the evolutionary medicine movement. Jimmy and Christine Moore - we stayed at the same hotel, so I got a chance to speak with them several times. Very sweet and enthusiastic - loved Jimmy's twitter coverage of the event. I felt for their recent losses. Paul and Shou Ching Jaminet - of course I've met them before, but I love talking to them so much I have to pull myself away to meet some of the non-Bostonians. Their combination of genius, humility, and gentle disposition is a terrific antidote to the typical slash and burn academic types.
At the conference proper I met a bunch more people: Julianne Taylor and her husband Mark, the other part of the New Zealand contingent. I loved talking to Julianne and Mark - and I love her clothes (actually, Mark was a very sharp dresser too). Danny Roddy, Chris Kresser's sidekick in the Healthy Skeptic Podcast - very nice young man who seemed to know everyone already, and introduced me to a lot of people. Dave Csonka was terrific and easy-going. J. Stanton was unsurprisingly intense and very tall! Lindsay Starke was as cute and smart as her @gone2croatan twitter feed would lead you to believe. It was great to hang out with her and with Andrew. Lex Rooker, famous for his raw paleo living, is actually the one who gave me a cookie. He told me it was a "paleo cookie" - but as I told Danny Roddy, I've been around the cookie block a few times, and I know a neolithic cookie when I see one. I'm sorry to say it tasted much better than the pemmican. Basil G from Atlanta brings knowledge together from Greece, the Atlanta Roller Derby scene, Emory University biologic sciences, and photography. I hope he and Jolly took only good photographs of me ;-)
On the second day of the conference, I spoke briefly to Tom Naughton, who surprised me by knowing who I was. I also met The Lazy Caveman… and my memory is failing me at this point. I'm sure I am leaving out someone very important.
The culinary high point (besides the steaks on the first night) had to be going to Animal with Dallas and Melissa Hartwig, Julianne Taylor and her husband Mark McNeill, and Jamie Scott on Friday night. I was able to sample some foods for the first time - including brains (which was sort of like a crispy succulent custard), pig's tail, and fried pig ear. Everything was excellent, but not gluten free. Dallas and Melissa defy definition - they are superlative with respect to health, vibrancy, beauty, drive, organization and intelligence. I was very delighted to spend time with them. I loved the dinner Saturday night, sitting at a table with 20 of the presenters and good friends. I was very happy to meet Rhys Southan of Let Them Eat Meat - his blog is consistent and excellent. Most from this dinner group (which included, among others, Durant, Guyenet, McEwan, Minger, Southan, and Masterjohn) were younger than I am - I felt like the paleo big sister (though they might be young enough that I could be their paleo mom). Our party was crashed by some enthusiastic protestors of the Rawsome raid that happened Thursday morning.
You've probably had enough of the name game, and I'm running out of positive adjectives - next post will be about Day 3 of the symposium - the MovNat one day seminar at Venice Beach.
I was very gratified and surprised to find two evolutionary medicine psychiatrists who had come to the conference and went out of their way to speak to me. We talked some shop and how to safely integrate evolutionary medicine principles - and how to document it, which in a medicolegal sense is absolutely key. They had some terrific ideas, and it was encouraging.
But the psychiatrists and the other people, the ones you know from the internets, they were amazing. Stephan Guyenet and Clifton Harski both noted in their most recent blog posts that overall it was a fit, attractive, and healthy-looking group. Obviously radical ancestral health enthusiasts will be self-selecting for health conscious people - but it was a stunning advertisement for the lifestyle. There was also, in general, a high level of positivism and intelligence.
Now some pictures - from my iphone 3GS, so don't expect too much.
 |
| Paul Jaminet and Danny Roddy |
 |
| John Durant, Lindsay and Dave Csonka in background. Shou-Ching Jaminet in foreground. |
 |
| Tall one is Dr. Eenfeldt, Chris Masterjohn, Stephan Guynet, Dave Csonka |
 |
| Robb Wolf |
 |
| Stephan Guyenet |
 |
| MovNat's Clifton Harski |
 |
| Denise Minger (sorry I caught you with your eyes closed!) |
 |
| Andrew (Evolvify), Lindsay, Jamie Scott |
 |
| Me trying pemmican |
 |
| Most shocking thing eaten at the ancestral health symposium |
 |
| Lindsay |
 |
| Jamie Scott and Dave Csonka |
 |
| Best Hair of the conference (was a close one with J. Stanton's long flowing mohawk) |
… I'm back. All right! Now the dirt! Just kidding. I just wanted to mention my impressions of the many I met - and if I skip you, I'm terribly sorry.
Jamie Scott - Awesome, humble fellow who came all the way out from New Zealand to help liven up my presentation and to meet and connect with the other AHS folks. I knew up front with the presentation we were going to have to hang out a bit, which can be a risk with someone you have never met. However, we were buddies from the get-go, and it was terrific to present with him and to show him around Los Angeles a little, as it was his first visit to the States. Jamie is a skeptic, as I am, and an excellent person to discuss ideas with. He also (fortunately) never seems to tire of talking paleo!
Folks from the presenter/volunteer party: Dr. BG - amazing, vibrant and gorgeous as we knew already. Down to earth and practical, which I actually wouldn't expect from her blogging, which is aways a cross between rock and roll, hotness, and amazing anthropology and pharmacology. Her sister was also very nice and gave me her extra chcocolate bar after my presentation. They both came to MovNat, and that was an amazing experience. Denise Minger - I had a chance to chat with her later on Saturday night, but I just have to echo everyone else's sentiments about her being bubbly and delightful. Richard and Bea Nikoley - who looked great, tanned, and were among the first (of many) to remark about how young I am. Let the record now show that I am 37. So younger than some, and older than many!
The Drs. Eades - formidable presence, lovely to talk to. I do admire their ability to practice the medicine they felt was right in the low-fat heyday of the 80s and 90s. Were I an obesity doctor back then, I would have lost my mind and wandered off into the wilderness. Bryan Barksdale - this young man is starting life as an MD/PhD student. Funnily enough, we both went to the same high school. Aaron Blaisdell and Brent Pottenger - I can only imagine the amount of work that went into organizing the symposium. Thank you, thank you, thank you. Andrew "Evolvify" - I still haven't got you figured out; I respect the genius and mostly just sit back and absorb the blog. He reminded me of some of my friends from back home in Austin, who tend to be brilliant and a bit off the beaten path. Stephan Guyenet - I hate to use the term "adorable" for him, but it describes him completely, from his relaxing zen personality to his amazing brain. I owe Stephan a lot as his blog helped me get a holistic head or tails of the evolutionary medicine piece - and his blog drives a lot of traffic to mine ;-)
Melissa McEwen and Chris Masterjohn I had met before, and I greatly admire their persistence in chasing down truth, and excellence in analysis of papers. John Durant and I had a discussion about writing books - his sounds well on its way. He's very down-to-earth and approachable. Clifton Harski and Erwan Le Corre - I will talk more about them in my MovNat post. Dr. Pendergrass had called me before to discuss the neuroregulation of obesity, he is not a blogger, but teaches biochemistry to med students, and is intense and enthusiastic about the evolutionary medicine movement. Jimmy and Christine Moore - we stayed at the same hotel, so I got a chance to speak with them several times. Very sweet and enthusiastic - loved Jimmy's twitter coverage of the event. I felt for their recent losses. Paul and Shou Ching Jaminet - of course I've met them before, but I love talking to them so much I have to pull myself away to meet some of the non-Bostonians. Their combination of genius, humility, and gentle disposition is a terrific antidote to the typical slash and burn academic types.
At the conference proper I met a bunch more people: Julianne Taylor and her husband Mark, the other part of the New Zealand contingent. I loved talking to Julianne and Mark - and I love her clothes (actually, Mark was a very sharp dresser too). Danny Roddy, Chris Kresser's sidekick in the Healthy Skeptic Podcast - very nice young man who seemed to know everyone already, and introduced me to a lot of people. Dave Csonka was terrific and easy-going. J. Stanton was unsurprisingly intense and very tall! Lindsay Starke was as cute and smart as her @gone2croatan twitter feed would lead you to believe. It was great to hang out with her and with Andrew. Lex Rooker, famous for his raw paleo living, is actually the one who gave me a cookie. He told me it was a "paleo cookie" - but as I told Danny Roddy, I've been around the cookie block a few times, and I know a neolithic cookie when I see one. I'm sorry to say it tasted much better than the pemmican. Basil G from Atlanta brings knowledge together from Greece, the Atlanta Roller Derby scene, Emory University biologic sciences, and photography. I hope he and Jolly took only good photographs of me ;-)
On the second day of the conference, I spoke briefly to Tom Naughton, who surprised me by knowing who I was. I also met The Lazy Caveman… and my memory is failing me at this point. I'm sure I am leaving out someone very important.
The culinary high point (besides the steaks on the first night) had to be going to Animal with Dallas and Melissa Hartwig, Julianne Taylor and her husband Mark McNeill, and Jamie Scott on Friday night. I was able to sample some foods for the first time - including brains (which was sort of like a crispy succulent custard), pig's tail, and fried pig ear. Everything was excellent, but not gluten free. Dallas and Melissa defy definition - they are superlative with respect to health, vibrancy, beauty, drive, organization and intelligence. I was very delighted to spend time with them. I loved the dinner Saturday night, sitting at a table with 20 of the presenters and good friends. I was very happy to meet Rhys Southan of Let Them Eat Meat - his blog is consistent and excellent. Most from this dinner group (which included, among others, Durant, Guyenet, McEwan, Minger, Southan, and Masterjohn) were younger than I am - I felt like the paleo big sister (though they might be young enough that I could be their paleo mom). Our party was crashed by some enthusiastic protestors of the Rawsome raid that happened Thursday morning.
You've probably had enough of the name game, and I'm running out of positive adjectives - next post will be about Day 3 of the symposium - the MovNat one day seminar at Venice Beach.